Leiomyoma of the Hand Mimicking a Pearl Ganglion
advertisement

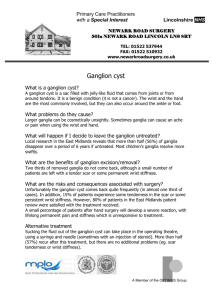
Case Report 134 Leiomyoma of the Hand Mimicking a Pearl Ganglion Wen-E Yang, MD; Swei Hsueh1, MD; Chih-Hua Chen, MD; Zhon-Liau Lee, MD; Wen-Jer Chen, MD Leiomyomas rarely occur in the hand. To our knowledge, there have been no reports of a leiomyoma of the hand mimicking a pearl ganglion in the English literature. We report such a case with a leiomyoma of the right third finger in a 59-year-old woman. The tumor was excised together with the underlying sheet of tissue. The pathology revealed that the tumor was linked to the underlying structure of a vascular wall by a stalk of tumor tissue. This report serves to remind clinicians to include leiomyoma in the differential diagnosis when encountering a 'ganglion-like lesion'. Also, this report demonstrates the link between a leiomyoma and its underlying origin. (Chang Gung Med J 2004;27:134-7) Key words: leiomyoma, pearl ganglion. L eiomyomas, which are benign tumors of smoothmuscle origin, rarely occur in the hand.(1,2) To our knowledge, there have been no reports of a leiomyoma of the hand mimicking a pearl ganglion in the English literature.(3) We describe such a case of a painful leiomyoma of the hand. bluish nodule with a firm, rubbery consistency arising from a vessel wall with a stalk connecting the nodule to the vessel wall structure. The nodule was 4 mm in diameter. Histological examination demonstrated a typical microscopic appearance of a leiomyoma with intertwining bundles of smooth-muscle cells, and no mitotic figure was seen (Fig. 1). CASE REPORT A 59-year-old woman presented with a painful nodule on her right long finger. Physical examination revealed a deeply seated nodular lesion about 5 mm in diameter, at the distal palmar crease of the right palm. The lesion was tender to palpation, and she had had pain on gripping for the previous 3 months. No other masses were detected in the hand or the upper extremity. With use of local anesthesia without a tourniquet, en bloc excision of the nodule was performed. A transverse incision was made in line with the distal palmar crease. The nodule together with the underlying sheet of tissue was excised. The wound was primarily closed using nonabsorbable monofilament sutures. Pathological analysis of the specimen revealed a smooth, discrete, Fig. 1 Photomicrograph showing the storiform architecture of spindle cells (H&E stain, Ű150). From the Department of Orthopedic Surgery, 1Department of Pathology, Chang Gung Memorial Hospital, Taipei. Received: Mar. 7, 2003; Accepted: Jun. 2, 2003 Address for reprints: Dr. Wen-E Yang, Department of Orthopedic Surgery, Chang Gung Memorial Hospital. 5, Fushing Street, Gueishan Shiang, Taoyuan, Taiwan 333, R.O.C. Tel.: 886-3-3281200 ext. 2163; Fax: 886-3-3278113; E-mail: yangwene@cgmh.org.tw 135 Wen-E Yang, et al Leiomyoma of the hand mimicking a ganglion Immunohistochemical staining for muscle-specific actin with the HHF 35 antibody revealed that the tumor was of a muscular origin (Fig. 2). At the 1year follow-up examination, there was neither evidence of local recurrence nor pain at the site of the excision. The patient had full range of motion of the wrist and fingers. There was no evidence of other masses elsewhere in the body. Fig. 2 Photomicrograph showing the brown-colored storiform architecture of spindle cells which reveals that the leiomyoma is of muscular origin. (immunohistochemical staining for muscle-specific actin, HHF35, Ű150). DISCUSSION Leiomyomas are benign tumors of smooth-muscle origin. Uterine leiomyomas are the most common tumors in women.(4) Leiomyomas of the hand are extremely rare and arise from non-striated muscles in the upper extremity, such as erector pilli, sweat glands, and vascular walls.(5) Most reports of leiomyomas of the hand have included only 1 or 2 patients each.(1,2,6-11) Uchida et al.(12) reported on 11 patients with a leiomyoma in the upper extremity. Neviaser and Newman reported 24 leiomyomas of the hand and forearm in their review of 85 vascular leiomyomas,(13) which we believe to be the largest series to date. However, none of these reports had any similarity to our case. The only report of a leiomyoma mimicking a pearl ganglion was in Polish.(3) In general, leiomyomas occur in the third and fourth decades of life.(4) The average age of patients with a leiomyoma in the hand was reported to be Chang Gung Med J Vol. 27 No. 2 February 2004 from 39 to 46 years.(12,13) These lesions are twice as common in women and girls as in men and boys; when they occur in the extremities, they are more common in the leg, ankle, and foot than in the upper extremity. (2) The most characteristic subjective symptom of a leiomyoma is tenderness that evolves into pain, which is often paroxysmal.(1) However, Uchida et al. reported that leiomyomas in the hand are usually not painful, but that lesions in the arm and the forearm commonly are. There is difficulty in differentiating a lesion like this case from a true pearl ganglion as both present as a tiny painful nodule. A possible preoperative diagnosis may require an expensive imaging study such as magnetic resonance imaging to differentiate the many possible other tumors of the hand. Operative excision is the treatment of choice in these cases for both pathologic diagnosis and for definite treatment. If an adequate margin is obtained, recurrence of a leiomyoma is rare.(1) There was no recurrence in this patient 2 years after the operation. Our findings are exceedingly unusual, not only because the leiomyoma developed in the hand, but also because of its similarity to a ganglion. To our knowledge, there has been no previous report of the occurrence of a leiomyoma mimicking a ganglion in the English literature. This report can serve to remind clinicians to include leiomyoma in the differential diagnoses when encountering a 'ganglion-like lesion'. This report also demonstrates the link between a leiomyoma and its underlying origin. REFERENCES 1. Duinslaeger L, Vierendeels T, Wylock P. Vascular leiomyoma in the hand. J Hand Surg[Am] 1987;12:624-7. 2. Robinson SC, Kalish RJ. Leiomyoma in the hand. A case report. Clin Orthop 1990;255:121-3. 3. Tyszka JJ, Stypulkowski TA, Bieniawska M. Leiomyoma diagnosed and treated as a ganglion. [in Polish] Chirurgia Narzadow Ruchu i Ortopedia Polska. 1987;52:402-4. 4. Robbins SL, Cotran RS, Kumar V. Pathologic Basis of Disease. Ed. 3, Philadelphia: W. B. Saunders Co., 1984: 1136-7. 5. Neviaser RJ, Adams JP. Vascular lesions in the hand. Current management. Clin Orthop 1974;100:111-9. 6. Bogumill GP, Sullivan DJ, Baker GI. Tumors of the hand. Clin Orthop 1975;108:214-22. 7. Duhig J T, Ayer JP. Vascular leiomyoma. A study of sixtyone cases. Arch Pathol 1959;68:424-30. 8. Firpo CA, Rimoldi MA, Bertole A. Leiomyomas of the Wen-E Yang, et al Leiomyoma of the hand mimicking a ganglion hand. Internat Surg 1976;61:45-6. 9. Hauswald KR, Kasdan ML, Weiss DL. Vascular leiomyoma of the hand. Case report. Plast Reconstr Surg 1975; 55:89-91. 10. Oughterson AW, Tennant R. Angiomatous tumors of the hands and feet. Surgery 1939;5:73-100. 11. Weisman PA. Blood vessel tumors of the hand. Plast Reconstr Surg 1959;23:175-86. 12. Uchida M, Kojima T, Hirase Y, Iizuka T. Clinical characteristics of vascular leiomyoma of the upper extremity: 136 report of 11 cases. British J Plast Surg 1992;45:547-9. 13. Neviaser RJ, Newman W. Dermal angiomyoma of the upper extremity. J Hand Surg 1977;2:271-4. 14. Boyd R, Bhatt B, Mandell G, Saxe A. Leiomyoma of the hand: a case report and review of the literature. J Hand Surg[Am] 1995;20:24-6. 15. Vaughn TR. Louton RB. Terranova WT. A large leiomyoma of the digit [letter]. Plast Reconstr Surg 1990;86:6056. Chang Gung Med J Vol. 27 No. 2 February 2004 137 1 59 (طܜᗁᄫ 2004;27:134-7) هࡔطܜᗁੰ έΔੰડ ࡊĂ1ঽநࡊ ͛͟צഇĈϔ઼92ѐ3͡7͟ćତצΏྶĈϔ઼92ѐ6͡2͟Ą ৶פ٩ОώĈ͛˘ᗁरĂهࡔطܜᗁੰ ࡊĄॿᎩ 333 ᐸ̋ฏೇᎸූ 5 ཱིĄ Tel.: (03)3281200 ᖼ 2163; Fax: (03) 3278113; E-mail: yangwene@cgmh.org.tw