assessment of attentional - Cambridge Brain Sciences
advertisement

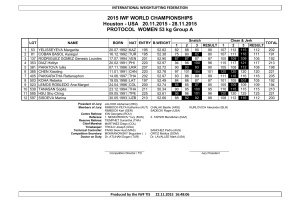
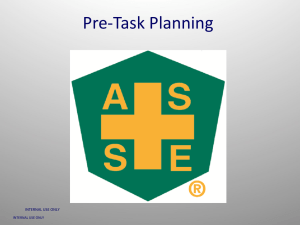
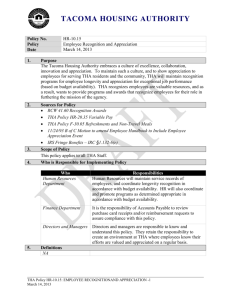
Psychopharmacology (1993) t 10: 395-401 Psychopharmacology © Springer-Verlag 1993 Further analysis of the cognitive effects of tetrahydroaminoacridine (THA) in Alzheimer's disease: assessment of attentional and mnemonic function using CANTAB Barbara J. Sahakian 1, Adrian M. Owen 1, Nicola J. Morant 2, Sarah A. Eagger 2, Stephen Boddington 2, Lissa Crayton 2, Helena A. Crockford 2, Maureen Crooks 2, Katie Hill 1, and Raymond Levy 2 1Department of Experimental Psychology, University of Cambridge, Downing Street, Cambridge CB2 3EB, UK 2Section of Old Age Psychiatry, Institute of Psychiatry, De Crespigny Park, Denmark Hill, London SE5 8AF, UK Received June 1, 1992 / Final version September 23, 1992 Abstract. Results of a placebo controlled cross-over trial (N = 89) of the anticholinesterase drug THA as a treatment for dementia of the Alzheimer's type (DAT) are reported, with reference to previous trials of the drug and the cholinergic hypothesis of aging and dementia. Using computerised tests sensitive to specific aspects of memory and attention, evidence is found for improvements in attentional function rather than memory, in patients with mild to moderate DAT. Although these improvements were significant, they were small and restricted to certain tests of attentional function. Nevertheless, they add to the growing body of evidence that the chotinergic system is involved in the control of attentional processes. The results will be relevant to future investigations into the therapeutic effects of enhancement of the cholinergic system in DAT sufferers. Key words: Tetrahydroaminoacridine (THA) - Dementia of the Alzheimer type (DAT) - Attention Memory CANTAB The cholinergic hypothesis of aging and dementia attributes cognitive impairments to reduced central cholinergic function (Drachman and Sahakian 1979). Critical evidence for this hypothesis is that the degree of cognitive impairment in patients with DAT is positively correlated with the decrease in choline acetyltransferase activity and a reduction in acetylcholine synthesis in brain tissue measured in post mortem and biopsy studies, respectively (Perry et al. 1978; Francis et al. 1985). Subsequently, there has been great interest in the possibility of a therapeutic strategy involving correction of the impairment in memory and cognitive function of DAT patients by enhancement of central cholinergic function. One way of making more acetylcholine available at central synapses is the inhibition of the breakdown of acetylcholine. This is one of the many actions of the drug tetrahydroaminoacridine (THA). Its other actions include monoamine oxidase inhibition (Kaul 1962), potassium channel blockade Correspondence to." B.J Sahakian (Drukarch et al. 1987) and interaction with subtypes of muscarinic and nicotinic receptors (Perry et al. 1988). There is a strong suggestion from the combined results of a number of experimental studies that parts of the central cholinergic system are involved in the control of attentional processes (see Dunnett et al. 1991 and Sahakian 1988 for reviews). Recent studies of neurotoxic lesions in rats causing extensive cholinergic cell loss indicate that cholinergic regulation of the neocortex may influence specific aspects of discrimination performance and visual attention (Dunnett et al. 1991). In addition, Warburton and Brown's work with rats (1971, 1972), using both the cholinergic antagonist scopolamine and the indirect cholinergic agonist physostigmine, suggest that cholinergic agents affect the processing of information input rather than learning and memory. Recent work by Sahgal et al. (1990) finding no effects of three cholinergic drugs (nicotine, oxotremorine and THA) on memory mechanisms in rats is consistent with this. Drachman et al. (1980) demonstrate that the effects of 1 mg of scopolamine given to young adults mirror the effects of aging in a dichotic listening task requiring high levels of attention and information processing. Sahakian et al. (1989) found that nicotine (which mimics the action of acetylcholine a t nicotinic receptor sites) improved performance of Alzheimer patients on tasks involving attention and information processing, but failed to improve performance in a task of short-term memory. There are several reports of improved performance in clinical trials of cholinergic drugs in patients with DAT (e.g. Christie et al. 1981; Belier et al. 1985). The degree of improvement is typically not large and is highly variable between doses and patients, probably reflecting the heterogeneity in the DAT population. Many of these studies are beset with problems of small sample sizes and poor design. Several clinical trials of THA have been conducted recently (e.g. Summers et al. 1986; Chatellier and Lacomblez 1990; Gauthier et al. 1990; Molloy et al. 1991). The many methodological problems of these trials have been discussed elsewhere (Eagger et al. 1991a, 1992). Nevertheless, it has been possible to find significant improvements on clinical rating scales (Eagger et al. 1991a, 396 b). H o w e v e r , of p r i m e c o n c e r n is t h a t specific effects o n m e m o r y o r a t t e n t i o n m a y r e m a i n u n d e t e c t e d in tasks w h i c h fail to s e p a r a t e t h e m o d a l i t i e s . I n the p r e s e n t s t u d y c o m p u t e r i s e d tests d e s i g n e d to test v e r y specific a s p e c t s o f m e m o r y a n d a t t e n t i o n are used. T h e s e h a v e b e e n s h o w n to be p a r t i c u l a r l y sensitive to t h e e a r l y stages o f n e u r o d e g e n e r a t i v e diseases s u c h as D A T ( S a h a k i a n et al. 1988) a n d also to the c h o l i n e r g i c a n t a g o n i s t , s c o p o l a m i n e ( R u s t e d a n d W a r b u r t o n 1988). T h e y h a v e the f u r t h e r a d v a n t a g e of b e i n g c o m p a t i b l e w i t h m a n y o f the p a r a d i g m s u s e d in a n i m a l r e s e a r c h (see D u n n e t t et al. 1991). Materials and methods Subjects Patients were selected from men and women of any age or race who met N I N C D S - A D R D A criteria for a diagnosis of probable Alzheimer's disease (McKhann et al. 1985). All subjects had a MiniMental State Examination (MMSE; Folstein et al. 1975) score in the range of 8 28 and a Clinical Dementia Rating (Hughes et al. 1982) of either I (mild dementia) or II (moderate dementia). Subjects were excluded if there was: (1) any evidence of concurrent illness (e.g. cerebral infarction, significant hepatic disease, clinical depression or any other significant psychiatric symptoms); (2) any concurrent medication likely to interfere with or confuse the interpretation of the expected action of THA; (3) no reliable caregiver who could ensure compliance with the protocol. Of the 89 patients who entered the study, 65 completed it. Most withdrawals were due to side-effects while on the active treatment. The commonest reason for withdrawal was an elevation of liver enzymes occurring in 12 patients (see Eagger et al. 1991a for further details). Those who withdrew from the study were not significantly different from those who completed it on any of the demographic of baseline measures. Statistical analyses are on the data from the 65 patients who completed the study. Des@n This was a randomised, double-blind placebo controlled cross-over study. Baseline assessments were followed by two 13-week treatment periods (period 1 and period 2) separated by a 4-week washout. Subjects were randomly assigned to either group A, (receiving active THA and active lecithin followed by placebo THA and placebo lecithin) or group B (receiving the treatments in reverse order). THA dosage was gradually increased over 4 weeks from 50 to 150 rag/day (up to a maximum tolerated dose). Neuropsychological and psychiatric assessments were made at the beginning, midpoint and end of each treatment period. Liver function and choline levels were also monitored carefully. Neuropsychological tests Initial assessment included the C A M C O G (Roth et al. 1986), to assess overall cognitive profile; the National Adult Reading Test (NART; Nelson 1982) as an estimate of premorbid IQ; and the shortened version of the WAIS (Wechsler 1955) as a measure of current IQ. Details of these are presented in Table 1. The data discussed in the present paper were obtained using the Cambridge Neuropsychological Test Automated Battery (CANTAB) tests of visual memory and attention. They use nonverbal stimuli and record responses using a touch sensitive screen linked to a BBC microcomputer. Subjects are familiarised with testing procedure by way of a "motor screening task" in which they are trained to point accurately at the screen. The CANTAB Visual Memory Battery comprises four tests (see Sahakian et al. 1988 for full details): 1. Pattern recognition. Subjects are presented with a series of coloured visual patterns. They are then required to indicate which of two simultaneously presented patterns they have seen before. 2. Spatial recognition. Subjects are presented with a series of five open white squares located in different positions on the screen. They are then required to indicate which position of two simultaneously presented boxes they have seen before. 3. Delayed matching-to-sample. After a delay of 0, 4, 8 or 16 s, subjects are required to pick the relevant matching stimulus from four possible choices comprising shape and colour distracters. A simultaneous matching condition is also run to control for perceptual deficits. 4. Conditional associative learning task. Six boxes around the screen open up one by one to reveal the location of different patterns. Each pattern then appears singly and subjects are required to indicate the appropriate location. If they fail to respond correctly, the pattern locations are shown again for up to ten trials. The task begins with only one stimulus pattern and progresses to two, three, six and finally eight patterns. The CANTAB attentional battery comprises four tests (see Downes et al. 1989 for full details of tests 1, 2 and 4) : 1. Following a simple rule and its reversal. Subjects are presented with a large and a small dot and required to point as quickly as possible to first the smaller dot for 20 trials and then the larger dot for the following 20 trials. The number of correct responses is recorded. 2. Attentional shift task. This has a similar rationale to the Wisconsin Card Sort Test (Berg 1948), in that it compares the capacity to make attentional shifts within the same stimulus dimension (intradimensional shift) with shifts to the currently non-attended dimension (extra-dimensional shift). Subjects are required to learn a series Table 1. Features at entry to trial (Patients completing study N = 65) Measure Age (yrs) Sex male} female} Memory impairment duration (yrs) Family yes} History no} Hughes CDR I} CDR II} CAMCOG MMSE AMTS ADL Full scale IQ" Verbal IQ" Performance IQ a Premorbid IQ b Premorbid verbal IQ b Premorbid perf IQ b Mean (range) 66.7 30 35 (52-84) 4.6 26 39 40 25 64.3 17.3 5.7 34.7 99.2 108.5 86.8 111.2 110.7 110.7 (1-10) Max possible score lII (31-96) (8-28) (2 9) (22-47) (61 150) (46 157) (48-140) (88-128) (85-129) (92 124) 107 30 10 47 a Using shortened form of the Wechsler Adult Intelligence Scale (Wechsler 1955) b Predicted using the National Adult Reading Test (Nelson 1982) 397 of discrimination tasks in which one of two stimuli is correct, on the basis of feedback provided by the computer following each choice. There are nine levels, presented in ascending difficulty and the level successfully attained is recorded. 3. Simple and choice reaction time test. There are five ascending levels of difficulty in this test, the first four of which act as training exercises to prepare subjects for the final level. At the first stage subjects simply have to touch the screen when a yellow dot appears in the centre, neither being too early nor too late. The choice reaction task is introduced at the second stage, with the dot now appearing in one of five locations. Subjects are introduced to the use of a touch pad at the third level. They are required to lift lheir hand from a touch pad as quickly as possible after a dot has appeared in a single location on the screen. This requirement to release the pad is combined with the requirement to touch the screen at the fourth level. Subjects are required to hold down the touch pad until a single dot appears in the centre of the screen and then to touch position of the dot as quickly as possible (see Fig. la). Subjects are now considered to be adequately trained for the fifth and final level, a five choice reaction time task. They are required to hold down the touch pad until the dot appears at one of five locations on the screen, and then point to the position on the screen where the dot was presented (see Fig. lb). At the first three stages, subjects are required to reach a criterion of 5/6 correct within 18 trials to go on to the next stage. At the fourth stage, subjects continue until a criterion 5/6 is reached or until 18 trials have been completed. At the fifth stage, subjects are given 40 trials to reach a criterion of 5/6 correct. Both accuracy (defined as the proportion correct at each stage) and speed of response are recorded for this test. For stages 4 (simple reaction time) and 5 (choice reaction time), the latter measure is divided into reaction time (latency to release touch pad) and movement time (from release of touch pad to touch of screen). In this study, comparisons were made between performance at stage 4, (single dot, release and touch) and stage 5, (5 locations, release and touch). 4. Complex visual search test. Subjects must match a stimulus presented in the centre of the screen with an exact equivalent presented simultaneously around the screen. Task difficulty is varied with the number of matching stimuli presented (1, 2, 4 or 8). There are 40 trials in total (10 at each level of complexity) and at each level, the total number of correct responses are recorded. Several standard paper-and-pencil tests of cognitive functioning were also administered: the Object Learning Test (KOLT) and Digit Copying Test (KDCT) from the Kendrick Cognitive Tests for the Elderly (Kendrick 1985); Digit Span (DS) and Digit Symbol Substitution (DSST) tasks from the Wechsler Adult Intelligence Scale (Wechster 1955); the Logical Memory subtest from the Wechsler Memory Scale - immediate and 30 min delay (Wechsler and Stone 1973); and the Benton Visual Retention Test - Administration A (Benton 1974). The three main clinical outcome measures were the Mini-Mental State Examination (MMSE, Folstein et al. 1975), the Abbreviated Mental Test Score (AMTS, Hodkinson 1972) and a carer's rating of activities of daily living (ADL, Lawton and Brody 1969). The Blessed Dementia Rating Scale (Blessed et al. 1968) and the Rosen Alzheimer's Disease Assessment Scale: non-cognitive sub-scale (Rosen et al. 1984) were also administered. Statistical m e t h o d o l o g y Analysis followed a two stage procedure for the analysis of cross over trials proposed by Hills and Armitage (1979). Each parameter was tested initially for differential carry-over effects of the first treatment across the washout period into the second treatment..This was done using a 2 x 2 analysis of variance (ANOVA) on the two treatment groups by the change in score over the treatment periods (ie endpoint minus baseline scores). If no carry-over effects were detected the treatment effect was tested using analysis of variance on all the data. However, if significant carry-over effects were detected, the treatment effect was tested using a one-way ANOVA on the change during treatment period 1. The test is thus reduced to an () Fig. la, b. The simple (a) and choice (b) reaction time tasks. Subjects are required to touch the circle in which the dot appears independent groups design. In either case, all data were analysed as change scores; that is, the change in score in the THA condition (end of treatment score - baseline score) versus the change in score in the placebo condition (end of treatment score - baseline score). A significance level of P _< 0.10 was used for the analysis of carryover effects. This was done because it was considered very important to detect even relatively small carry-over effects, and because the test is based on between subject differences and is therefore less powerful than the treatment effect test based on within subject differences. All analyses were performed using the SPSS-PC + package. Results T H A h a d n o significant effects o n the c o m p u t e r i s e d tests of p a t t e r n a n d spatial r e c o g n i t i o n , d e l a y e d m a t c h i n g to s a m p l e or p a i r e d associates c o n d i t i o n a l learning. In o r d e r to illustrate these n e g a t i v e data, the results f r o m the test of s i m u l t a n e o u s a n d d e l a y e d m a t c h i n g to s a m p l e are presented in Fig. 2. T h e r e was n o difference b e t w e e n the T H A c o n d i t i o n a n d the p l a c e b o c o n d i t i o n a l t h o u g h in b o t h g r o u p s t h e r e was a significant d e l a y - d e p e n d e n t deficit [F(3,183) = 19.25, P < 0.0001]. By c o m p a r i s o n w i t h the n o r m a l c o n t r o l subjects assessed by S a h a k i a n e t a l . (1988; see Fig. 2) it is clear t h a t whilst this test is n o t sensitive to the effects of T H A in D A T , it is c e r t a i n l y sensitive to the disease itself. T h i s lack of effect is clearly n o t d u e to a f l o o r effect as the m e a n v a l u e s w e r e well a b o v e c h a n c e level (25%). In the m o r e t r a d i t i o n a l p a p e r a n d pencil tests a s s u m e d to m e a s u r e m e m o r y capacity, s h o r t t e r m m e m o r y a n d learning, t h e r e w e r e also n o significant effects of the drug. 398 100 t 0 90] • 80 ] [] 0,08 - 0.06 - i.. 9 0 0 i. 0 0 7O . ~ / D aO- 0.04 " cO t,. 0 O - 0.02 Q. ¢,- 50 ¸ t= 40. 0,00 !ii!iii;iiiiiiiiiiiii!iiiiiiiiiiiiiiiiiiiiiiiiiiiiiii cO 30- ........................................ -0.02 - chance level Delay (secs) -0.04 THA Fig. 2. The mean percentage correct scores in the simultaneous (SIM) and delayed (0 16 s) matching to sample task. Whilst this memory task is clearly not sensitive to the effects of THA, significant deficits are evident in patients with DAT when compared to normal controls (Sahakian et al. 1988b) (- O ) Controls; ( • ) THA; ( [ ] - ) placebo In contrast, there were a number of significant differences between the drug and placebo conditions on certain of the computerised tests of attentional abilities. Specifically, in the test of simple and choice reaction time there were differences between the two tasks in terms of both speed and accuracy of responding. In terms of simple reaction time accuracy, there was no significant interaction between treatment (THA or placebo) and time (baseline to end of treatment) [F(1,59) = 0.06, P > 0.05]. In contrast, in the choice reaction time condition, there was a significant difference across the two treatment conditions [F(1,57) = 5.26, P < 0.05]. In Fig. 3, the mean change in the overall proportion of correct responses in the T H A and placebo conditions are presented. The mean change in the T H A condition was, in fact, significantly positive, overall, 50% of patients deteriorated in this condition compared to 68% in the placebo condition. Among the patients who became quicker on THA, average improvement was approximately 16% (mean scores = 0.68-0.85 correct). In terms of simple reaction time latency, there was again, no significant interaction between treatment and time [F(1,37)= 0, P > 0.05]. In contrast, in the choice reaction time condition, differences emerged in terms of both reaction time and movement time. In Figs 4 and 5, mean changes in reaction time (Fig. 4) and movement time (Fig. 5) in the T H A and placebo conditions are presented. For the reaction time measure, there was a significant interaction between treatment and time [F(1,33)= 9.23, P < 0.005]. The overall mean change was positive in the Placebo Condition Fig. 3. The mean change in the overall proportion of correct responses whilst in the THA and placebo conditions 0.4- ~o o ~no ® .~ ,_ :O 0.2- O.O -0.2 -0.4 - -0.6 " .8 ,-° o ee- -0.8 - -1.0 • e- o ,~" -1.2 ' -1.4 Placebo THA Condition Fig. 4. The mean change in choice reaction time in the THA and placebo conditions 399 0,2o o 0 O) ltl 0,0 I-It" ¢~1 -0.2 i!•i•ii•i!}•i!ii•i!i!i!i•i!i!i!•i•i!i•i•i!i•i•i•i•i•i•i•ii i•i!i!i!•i!i!i!•!i!i!i!i•i•i•i!i!i•i•i!ii•i•i•i•i•i•ii•i•ii)• E -0,4 > 0 -0.6 ~!~i!i~i!~iiiii~~i~iii~~i!;i!~i~;i!i!ii!i!~ii!i~i!iiii!~i!i!i~!ii!ii!~ii!i~iii~~i!~i~i~iii~~iiii~~i1~i i!;ii~ii~!~i~i~i~ii~i!~i~ ~i~ii~i~i i~!ii i~i~i!!ii i~i i i i i i i !!i!!ii!!ii ~!ii ~i~i~i i i!i iiiiil;iiiiil;iii:i;iiii:i;ii~i;i:i~N~ E 0 -0.8 .~_ ,~ liNiiiiiiiii#iiiiiiiiiNi!iiiiiiiiii -1.0 it!iiii}iii;i~iii;i~i~iii;i!i!iiii;iiiiiiiii~iiiiii~iiiiii!iiiiii ¢o ¢- -1.2 -1.4 THA Placebo Condition Fig. 5. The mean change in choice movement time in the THA and placebo conditions T H A condition with no significant change in the placebo condition (see Fig. 4). Importantly, only 18% of patients became slower during the THA condition whilst 67% became slower during the placebo condition. Among the patients who actually became quicker on THA, average improvement was approximately 17% (from 0.64 to 0.53 s). Similarly for the movement time measure, there was a significant interaction between treatment and time [-F(1,33) = 5.97, P < 0.05]. The overall mean change was positive in the T H A condition with no significant change in the placebo condition (see Fig. 5). Again, only 6% of patients became slower in the T H A condition compared to 67% on placebo. Among those patients who actually improved on THA, average improvement was approximately 13% (from 0.84 to 0.73 s). When reaction time and movement time were combined into one overall measure of response latency, there was a highly significant interaction between treatment condition and time [F(1,33) = 14.6, P < 0.001]. Thus, in terms of speed of responding, T H A had a significant beneficial effect in measures of both movement time and reaction time in the choice condition, but had no effect on simple reaction time. In the test designed to assess the patients' ability to follow a simple rule and to reverse that rule, there was a significant interaction between condition and time IF(l,15) = 9.62, P < 0.01]. In the T H A condition, only 16% of patients deteriorated on this task compared to 26% in the placebo condition. Among those that became more accurate on THA, average improvement was 8% (from 33.6 correct dots to 36.28 correct dots). However, T H A did not improve all forms of attentional dysfunction. I~n the visual discrimination learning task designed to assess set-shifting ability there was no difference in the mean scores for stage reached in the T H A condition I-weT H A s t a g e - - 4 . 3 2 (0.37), post-THA stage = 4.61 (0.38)] and the placebo condition [pre-placebo stage ='4.37 (0.4), post placebo stage = 4.59 (0.4)]. Similarly, in the complex visual search test, the mean total correct score (maximum = 40) did not differ in the THA condition [-pre-THA score = 38.08 (1.2), post-THA score = 39.34 (1.23)] and the placebo condition [we-placebo score = 37.57 (1.25), post-placebo score = 37.63 (1.4)]. In summary, significant effects of THA were only found for the computerised tests of choice reaction time and simple rule learning, with no other results approaching significance. For comparison with the effects found with computerised testing, analysis of the three main clinical outcome measures showed statistically significant effects of the drug on the M M S E [-F(1,64) = 28.77, P < 0.0001] and AMTS [F(1,64)= 16.61, P = 0.0001], but not the ADL [F(1,64) = 0.09, P = 0.764]. The relative lack of effect on the ADL score did not appear to reflect the known insensitivity of this instrument in mild and moderate DAT since no significant change was observed even when only those patients with MMS scores of 15 or less were included in the analysis [F(1,35) = 0.756, P = 0.39]. None of the other psychiatric measures showed significant improvements under THA. These clinical outcome measures have been described in great detail by Eagger et al. (1991a). In order to identify features which might predict a good response to THA on the computerised tests of attention, Pearson product moment correlation coefficients were calculated between the change scores (on T H A and placebo) for these tests and changes on the M M S E and AMTS clinical outcome measures. No significant correlations were observed. In addition, no other patient characteristics, including age, age of onset, duration of illness, initial IQ or disease severity correlated with response on these tasks. Discussion Analysis of the specific tests of memory and attention reported here show that the statistically significant effects of T H A in DAT patients occurred on attentional tasks. Thus, the cognitive effects of this acetylcholinesterase inhibitor are most evident on some aspects of information processing and attentional function, rather than mnemonic performance. This supports other evidence, (Sahakian et al. 1989; Dunnett et al. 1991), that activity in the cortical cholinergic system helps to control attentional processes. Not only do these results enhance our understanding of the mechanisms involved, but they are also consistent with the report of an advantage of T H A over placebo on the psychiatric rating scales M M S E and AMTS. The effect of T H A on performance on the choice reaction time task was small but significant, both for 400 latency and accuracy indices of performance. In terms of accuracy 50% of patients improved with THA compared to 32% for placebo. However, there were insufficient numbers of particular types of errors to allow a detailed analysis of whether the drug was exerting its significant improvement by reducing errors of commission or omission or preventing premature responses. Latency scores improved in 82% and 94% of cases under THA compared to 33% and 38% in controls for reaction time and movement time, respectively. This improvement in both speed and accuracy means that patients treated with THA were not simply trading speed for accuracy. The effects on the five choice reaction time task were paralleled by a significant improvement on following a simple rule and its reversal task. Evidently the drug improved performance in the ability to follow an explicit rule, suggesting that it was improving attention to the task requirements. However, THA failed to improve all forms of attentional function. Thus the capacity to deduce rules on the basis of reinforcing feedback and to use them to solve simple discrimination tasks including shifting across stimulus dimensions was not improved by THA. In contrast to the other attentional tasks, this test does have a small working memory component. The ability to perform a visual search task in which subjects were required to match complex visual stimuli was also unimproved by THA. Finally, THA was unable to improve any of the measures of visual recognition memory and learning. Therefore, it is evident that the therapeutic efficacy of THA on cognition as measured by objective neuropsychological tests is somewhat limited. Although it is difficult to equate tests, it is important to note that the main effects in this study were limited to simpler tests of attentional function. Compared, for example, to the test of delayed matching to sample (see Fig. 2), where normal elderly controls generally score between 80 and 90%, control performance on both the choice reaction time task (96% correct) and the test designed to test simple rule learning ability (97% correct) is somewhat superior (Sahakian et al. unpublished observations). Performance on the more complex variants of these tests or on the tests of mnemonic or learning ability was not improved with THA. In support of the pattern of results with CANTAB, when the components of the Rosen Alzheimer's Disease non-cognitive scale (Rosen et al. 1984) were-analysed, the only subscore showing a significant advantage of THA was "concentration/distractibility" [F(1,63) = 5.55), P = 0.022]. This item measures how much the patient is distracted by irrelevant stimuli and/or must be reoriented to the ongoing task because of loss of train of thought. Consistent with this is anecdotal evidence from carets, many of whom noted that the effect of THA was to make patients more alert. Although these findings are clearly less precise than those obtained on the computerised batteries, they are consistent with our hypothesis that the effect of THA is primarily on attentional processes. The results reported here demonstrate typically small improvements on THA. Many previous studies investigating the possible therapeutic effects of THA in Alzheimer's disease report negative findings (although more promising results have recently been presented by Warner-Lambert in the US [FDA Advisory Committee Meeting for Peripheral and Central Nervous System Drugs: March 15, 1991]). Molloy et al. (1991) suggest that one reason why cholinergic based treatments in DAT are not as effective as would be theoretically expected, is that the drug is acting within the context of significant deficits in other neurotransmitter systems. This may of course be true especially in the more moderate or severe stages of the disease, where significant neuropathological changes may be evident. As well as employing a sufficiently rigorous design, and patients in the mild to moderate stages of the disease, the present research is unique in that it employs highly sensitive tests designed specifically to measure aspects of memory and attention separately. Thus, in previous studies, the CANTAB battery has been shown to be sensitive to the early effects of DAT and Parkinson's disease and other disorders (Sahakian et al. 1988; Downes et al. 1989) as well as to the effects of the muscarinic antagonist, scopolamine (Rusted and Warburton 1988). Part of the rationale for this battery is based on the comparison with findings from the animal neuropsychological literature, which thus enhances our understanding of the possible neuroanatomical and neurochemical mechanisms involved. It is relevant that THA has recently been found to have little effect on performance in a delayed matching to position test (Sahgal et al. 1990). The five choice reaction time task is analogous to a test used by Robbins et al. (1989) in rats with lesions of the substantia innominata which reduced cortical choline acetyltransferase activity by up to 50%. Deficits in both accuracy and speed of response were found. Although these may not have resulted from damage specifically to cholinergic cells, recent findings have strongly suggested that there is an important cholinergic component to the deficits, which can be reversed by the anticholinesterase physostigmine and by cholinergically enriched grafts (Muir et al. 1992). These results are of special significance in view of the previous resistance of cognitive decline in DAT to pharmacological treatment. This suggests that such an approach to treatment may still prove viable for cases in the mild to moderate stages of the disease. It remains to be seen whether other drugs of this class currently being developed will be able to produce larger effects, possibly including improvements in other areas of cognition. In conclusion, the present study has found evidence of improvements in certain aspects of attentional function with THA in mild to moderate cases of DAT. The clinical relevance of these improvements, given the possible side effects, remains a matter for individual clinical judgement. These data, obtained in a carefully controlled study of a large number of DAT patients, will also clearly provide important comparative data for future investigations of putative cognitive enhancing drugs in DAT sufferers. Acknowledgements. We wish to thank Parke Davis, Division of Warner lambert Company for support and Prof. Brian J Everitt for expert statistical advice. We also thank Dr. TW Robbins for his helpful comments on the manuscript. The CANTAB tests were developed with the assistance of a major award from the Weltcome Trust to Drs. TW Robbins, Barry J Everitt and BJS. BJS thanks The Eleanor Peel Foundation and The Wellcome Trust for support. 401 References Belier SA, Overall JE, Swarm AC (1985) Efficacy of oral physostigmine in primary degenerative dementia: a double-blind study of response to different dose level. Psychopharmacology 87 : 147-151 Benton AL (1974) Revised visual retention test, clinical and experimental applications. The Psychological Corporation, New York Berg EA (1948) A simple objective test for measuring flexibility in thinking. J Gen Psychol 39 : 15 22 Blessed G, Tomlinson BE, Roth M (1968) The association between quantitative measurements of dementia and the senile changes in the cerebral grey matter of elderly subjects. Br J Psychiatry 114:797-811 Chatetlier G, Lacomblez L (1990) Tacrine (tetrahydroaminoacridine; THA) and lecithin in senile dementia of the Alzheimer type: a multicentre trial. Groupe Francais d'Etude de la Tetrahydroaminoacridine. BMJ 300 : 495-499 Christie JE, Shering A, Ferguson J, Glen AIM (1981) Physostigmine and arecoline: effects of intravenous infusions in Alzheimer presenile dementia. Br J Psychiatry 138:46 50 Downes J J, Roberts AC, Sahakian BJ, Evenden JL, Morris RG, Robins TG (1989) Impaired extra-dimensional shift performance in medicated and unmedicated Parkinson's disease: evidence for a specific attentional dysfunction. Neuropsychologia 27:1329 1343 Drachman DA, Sahakian BJ (1979) Effects of cholinergic agents on human learning and memory. In: Barbeau A, Growdon JH, Wurtman RJ (eds) Nutrition and the brain, vol 5. Raven Press, New York, pp 351 366 Drachman DA, Noffsinger D, Sahakian BJ, Kurdziel S, Fleming P (1980) Aging, memory, and the cholinergic system: A study of dichotic listening. Neurobiol Aging 1 : 39-43 Drukarch B, Kits KS, Van-der-Meer EG, Lodder JC, Stoof JC (1987) 9-Amino-l,2,3,4-tetrahydroacridine (THA), an alleged drug for the treatment of Alzheimer's disease, inhibits acetylcholinesterase activity and slow outward K + current. Eur J Pharmacol 141 : 153 157 Dunnett SB, Everitt BJ, Robbins TW (1991) The basal forebraincortical cholinergic system: interpreting the functional consequences of excitotoxic lesions. TINS 14 [11] :494-501 Eagger SA, Levy R, Sahakian BJ (1991a) Tacrine in Alzheimer's disease. Lancet 337 : 989-992 Eagger SA, Morant NJ, Levy R (1991b) Parallel group analysis of the effects of Tacrine versus placebo in Alzheimer's disease. Dementia 2 : 207-211 Eagger SA, Morant NJ, Levy R, Sahakian BJ (1992) Tacrine in Alzheimer's disease. Time course of changes in cognitive function and practice effects. Br J Psychiatry 160:36~40 Folstein MF, Folstein SE, McHugh PR (1975) "Mini-Mental State": a practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 12:189 198 Francis PT, Palmer AM, Sims NR, Bowen DM, Davison AN, Esiri MM, Neary D, Snowdon JS, Wilcock G K (1985) Neurochemical studies of early onset Alzheimer's disease: possible influence on treatment. N Engl J Med 313:7 11 Gauthier S, Bouchard R, Lamontagne A, et al. (1990) Tetrahydroaminoacridine-lecithin combination treatment in patients with intermediate-stage Alzheimer's disease. Results of a Canadian double-blind, crossover, multicenter study. N Engl J Med 322:1272-1276 Hills M, Armitage P (1979) The two-period cross-over clinical trial. Br J Clin Pharmacol 8:7-20 Hodkinson HM (I972) Evaluation of a mental test score for the assessment of mental impairment in the elderly. Age Ageing 1 : 233 239 Hughes CP, Berg L, Danziger WL, Coben LA, Martin RL (1982) A new clinical scale for the staging of dementia. Br J Psychiatry 140 : 566-572 Kaul P (1992) Enzyme inhibiting action of tetrahydroaminoacridine and its structural fragments. J Pharm Pharmacol 14:243-248 Kendrick DC (1985) Kendrick cognitive tests for the elderly. NFERNelson, Windsor, Berks Lawton MP, Brody EM (1969) Assessment of older people: selfmonitoring and instrumental activities of daily living. Gerontologist 9:179 186 McKhann G, Drachman D, Folstein M, Katzman R, Price D, Stadlan EM (1985) Clinical Diagnosis of Alzheimer's disease: Report of the NINCDS-ADRDA Work Group under the auspices of the Department of Health and Human Services Task Force on Alzheimer's Disease. Neurology 34:939-944 Molloy DW, Guyatt H, Wilson DB, Duke R, Rees I2, Singer J (1991) Effect of tetrahydroaminoacridine on cognition, function and behaviour in Alzheimer's disease. Can Med Assoc J 144:29 34 Muir JL, Dunnett SB, Robbins TW, Everitt BJ (1992) Attentional functions of the forebrain cholinergic systems: effects of intraventricular hemicholinium, physostigmine, basal forebrain lesions and intracortical grafts on a multiple-choice serial reaction time task. Exp Brain Res 89:611-622 Nelson HE (1982) National adult reading test manual. NFERNelson; Windsor, Berks Perry EK, Tomlinson BE, Blessed G, Bergman K, Gibson PH, Perry RH (1978) Correlations of cholinergic abnormalities with senile plaques and mental test scores in senile dementia. BMJ 2:1457 1459 Perry EK, Smith CJ, Court JA, Bonham JR, Rodway M, Atack JR (1988) Interaction of 9-amino-l,2,3,4-tetrahydroaminoacridine (THA) with human cortical nicotinic and muscarinic receptor binding in vitro. Neurosci Lett 91:211-216 Robbins TW, Everitt BJ, Marston HM, Wilkinson J, Jones GH, Page KJ (1898) Comparative effects of ibotenic acid- and quisqualic acid-induced lesions of the sustantia innominata on attentional function in the rat: further implications for the role of the Cholinergic neurons of the nucleus basalis in cognitive processes. Behav Brain Res 35:221 240 Rosen WG, Mohs RC, Davis KL (1984) A new rating scale for Alzheimer's disease. Am J Psychiatry 141 : 1356-1364 Roth M, Tym E, Mountjoy C et al. (1986) CAMDEX: a standardised instrument for the diagnosis of mental disorder in the elderly with special reference to the early detection of dementia. Br J Psychiatry 149:698-709 Rusted JM, Warburton DM (1988) The effects of scopolamine on working memory in healthy young volunteers. Psychopharmacology, 96:145-152 Sahakian BJ (1988) Cholinergic drugs and human performance. In: Iversen LL, Iversen SD, Snyder SH (eds) Handbook of psychopharmacology, vol 20. Plenum Press, New York, pp 393-424 Sahakian BJ, Morris RG, Evenden JL, Heald A, Levy R, Philpot M, Robbins TW (1988) A comparative study of visuospatial memory and learning in Alzheimer-type dementia and Parkinson's disease. Brain 111:695 718 Sahakian BJ, Jones G, Levy R, Gray J, Warburton D (1989) The effects of nicotine on attention, information processing and short-term memory in patients with dementia of the Alzheimer type. Br J Psychiatry 154:797 800 Sahgal A, Keith AB, Lloyd (1990) Effects of nicotine, oxotremorine and 9-amino 1,2,3,4-tetrahydroacridine (tacrine) on matching and non-matching to position in rats: no evidence for mnemonic enhancement. J Psychopharmacol 4:210-218 Summers WK, Majovski LV, Marsh GM, Tachiki K, Kling A (1986) Oral tetrahydroaminoacridine in long-term treatment of senile dementia, Alzheimer type. N Engl J Med 315 : 1241-1245 Warburton DM, Brown K (1971) Attenuation of stimulus sensitivity induced by scopolamine. Nature 230:126-127 Warburton DM, Brown K (1972) The facilitation of discrimination performance by physostigmine sulphate. Psychopharmacologia 27 : 275 284 Wechsler D (1955) Manual for the Wechsler Adult Intelligence Scale. The Psychological Corporation, New York Wechsler D, Stone CP (1973) Manual Wechsler Memory Scale. The Psychological Corporation (copyright The Journal Press), New York