Abeer Ahmed Mohamed Shoman_candisartan..doc
advertisement

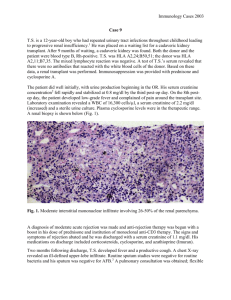
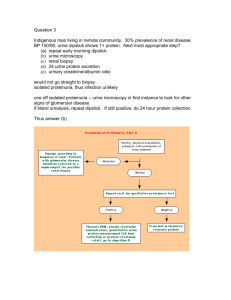
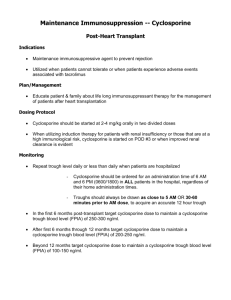
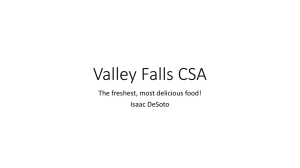
THE POSSIBLE PROTECTIVE ROLE OF CANDISARTAN ON CYCLOSPORINE INDUCED NEPHROTOXICITY IN RATS By Hanan T. Emam M.D.1, Abd El Moneim G. Madbouly M.D.2, Abeer A. Shoman M.D.3 and Noha. I. Hussein M.D3 1 Department of Pharmacology & Therapeutics, 2Department of Forensic & Toxicology and 3 Department of physiology, Faculty of Medicine, Benha University, Egypt ABSTRACT Cyclosporine A (CsA), a fungal undecapeptide, is the most common immunosuppressive drug used in organ transplantation and autoimmune diseases. However, nephrotoxicity is the major adverse effect of CsA use. The molecular mechanisms of CsA nephrotoxicity are not well characterized, but more recent studies suggest an involvement of angiotensin ll (ANG II) and reactive oxygen species in the development of cyclosporine nephrotoxicity. This study was thus designed to investigate the role of angiotensin II type I (AT1) receptor antagonist, candisartan,on CsA- induced nephrotoxicity. Three groups of rats were employed in this study; group 1 served as control, group 2 rats were treated with CsA (20mg/kg/day subcutaneously) for 21 days, and group 3 received CsA along with candisartan (1mg/kg/day perorally) 24 hr before and 21 days concurrently. Renal blood flow (RBF) was estimated by flowometer. Estimation of plasma renin activity serum creatinine, blood urea and tissue malondialdehyde content by using colorimetric methods. Renal tissue specimens were histopatholgically examined by hematoxylin & eosin staining. CsA administration for 21 days resulted in a marked renal impairment and significantly decreases (RBF), deranged the renal functions as well as renal morphology. All these factors were significantly improved by candisartan. These results clearly demonstrate the pivotal role of (AT1) receptor antagonist candisartan in CsA- induced nephrotoxicity. Keywords: Cyclosporine, Nephrotoxicity, Candisartan, Angiotensin, Renin. 1 INTRODUCTION Due to its potent immunosuppressive effects, cyclosporine (CsA) has improved allograft survival in organ transplantation and has been applied increasingly with considerable clinical benefit in the treatment of autoimmune diseases. Unlike most other immunosuppressive agents, cyclosporine has no depressant effects on the bone marrow. However, the therapeutic benefits of cyclosporine have been frequently limited by the occurrence of acute and chronic nephrotoxicity, which is the most serious common side effect. Cyclosporine nephrotoxicity therefore remains an important clinical challenge (1). It has been suggested that activation of the renin-angiotensin system is involved in the pathogenesis of CsA-induced nephrotoxicity (2). Angiotensin receptor blocker (ARB) as Irbisartan is effective in preventing CsA- induced vascular and renal adverse effects (2). Candisartan Cilexetil; an inactive ARB prodrug, which hydrolyzed to active form during absorption from GLT, due to its tight binding to AT, receptor it has longer activity than other members of ARBs (3). 2 MATERIALS AND METHODS Animals Twenty four male adult albino rats of locally breaded strain weighing between 150-250g at the beginning of the study were used. They have acclimatized for one week in groups (8/cage) in fully ventilated room at ordinary room temperature in pharmacology department, Benha Faculty of Medicine . Rats were allowed to ad libitum, access to water and balanced diet All experimental protocols were approved by the committee of Benha University during September 2012. At the beginning of the experiment they were divided into 3 groups each contained 8 rats: * Study groups: Rats were randomly divided into 3 groups, each of them consisted of 8 rats. Group 1: Control normal rat. Group 2: (cyclosporine nephrotoxic group): Rats of this group received cyclosporine in a dose of 20 mg/kg daily SC for 21 days(4). Group 3 (candisartan treated group): Rats of this group given the same dose of cyclosporine for 21 days along with candisartan 1mg/kg daily orally, 24 hour before and 21 days concurrently with cyclosporine treatment (4). All drugs and chemicals were freshly prepared before each experiment. All groups were subjected to the following investigation: 1. Renal blood flow (5) by Doppler flow meter. 3 2. Estimation of plasma renin activity (6). 3. Estimation of blood urea (7). 4. Estimation of serum creatinine (8). 5. Estimation of tissue malondialdehyde (MDA)content. (9). 6. Hitopathological studies (4). At the end of the experiment, rats were anaesthized with urethane (0.6 ml/100 gm of 25% freshly prepared solution), of about the abdominal cavity was opened, blood sample were collected from abdominal aorta and processed for biochemical measurements.the kidneys were exposed, removed and divided into 2 parts.one part was placed in 10% formaline for histopathological examination. The second part was kept at -70C and used for biochemical measurement of MAD. Statistical Analysis: All data were expressed as mean S.E, data were evaluated by the one way analysis of variance. Difference between groups were compared by Student's t-test with P 0.05 selected as the level of statistical significance (10). 4 RESULTS Effect of candisartan on cyclosporine induced nephrotoxicity in rats: a) The effect on RBF: There was significant (P < 0.05) reduction of RBF from a mean of 9.4 1.13 cm/s in control normal rats to a mean of 4.140.11 cm/s in rats received cyclosporine only table (1). (Fig. 1, 6, 7). RBF was significantly increased from a mean of 4.14 0.11cm/s in cyclosporine treated rats to a mean of 8.02 0.6cm/s in candisartan treated group. Table (1). (Fig. 1, 7& 8). b) Plasma renin activity: The mean value of plasma renin activity in control normal rats was 1.50 0.06 ng/ml/h. In rats received cyclosporine only this value was significantly elevated (P < 0.05) to reach 4.37 0.08 ng/ml/h. The mean value of plasma renin activity in candisartan treated group was insignificantly increased (P 0.05) to 4.58 0.09 ng/ml/h in comparison to the corresponding value of cyclosporine treated rats, table (1) (Fig. 2). c) Blood urea level: The mean value of blood urea level in control normal rats was 20.42.1 mg/dl. In rats received cyclosporine only this value was signficiantly elevated (P < 0.05) to reach 49.8 4.2 mg/dl. The mean value of blood urea level in candisartan treated group was significantly decrease (P < 0.05) to 31.82.2 mg/dl, in comparison to the corresponding value of cyclosporine treated rats, (Table 1) (Fig. 3). 5 d) Serum creatinine level: The mean value of serum creatinine level in control normal rats was 0.500.06 mg/dl. In rats received cyclosporine only this value was significantly elevated (P < 0.05) to reach 1.38 0.08 mg/dl. The mean value of serum creatinine level in candisartan treated group was significantly decreased (P < 0.05) to 0.58 0.06 mg/dl in comparison to the corresponding value of cyclosporine treated rats, table (1) (Fig. 4). e) Tissue MDA level; The mean value of MDA level in control normal rats was7.500.06 µM/g. In rats received cyclosporine only this value was significantly elevated (P < 0.05) to reach16.38 1.8 µM/g. The mean value of MDA level in candisartan treated group was significantly decreased (P < 0.05) to 10.58 1.06 µM/g in comparison to the corresponding value of cyclosporine treated rats, table (1) (Fig. 5). f) Histopathological examination: Renal sections of control group showed normal glomeruli & tubules and absence of any calcification (Fig. 9). It was noticed that cyclosporine induced tubular degeneration and vaculation, hyalinosis of basement membrane of glomeruli and renal tubules. Also, there was patchy dystrophic calcification at the corticomedullary junction and in the dilated tubules indicating nephrocalcinosis (Fig. 10 & 11). In the candisartan treated rats, the rats, the hyaline degeneration of tubular and glomeular basement membrane was markedly decreased, tubular atrophy and vaculation was much less evident. No calcification 6 was found in the renal interstitium or in the tubules with treatment (Fig. 12 &13). Table (1): Mean S.E.M. of RBF cm/s, Plasma renin activity ng/ml/h. blood urea level, serum creatinine level in mg/dl and tissue MDA level µM/g. in control group, cyclosporine nephrotoxic group and candisartan treated group (n = 8). Groups Group 1 (control group) 9.40.08 Group 2 (cyclosporine nephrotoxic group) 4.140.11* Group 3 Candisartan treated group 8.020.6** 1.50.06 4.37 0.08* 4.580.09# 20.42.1 49.84.2* 31.82.2** 0.5 0.06 1.38 0.08* 0.58 0.06** 7.50.6 16.381.2* 10.581.06** Parameters RBFcm/s Plasma renin activity ng/ml/h. Blood urea level mg/dl Serum creatinine mg/dl Tissue MDA level µM/g. *: Significant compared to control group. **: Significant compared to cyclosporine nephrotoxic group. #: In significant compared to cyclosporine nephrotoxic group. 7 12 10 ** 8 Group 1 6 Group 2 Group 3 * 4 2 0 RBF cm/s Fig. (1): A histogram showing the effect of candisartan treatment on RBFcm/s compared to cyclosporine nephrotoxic group 5 4.5 * # 4 3.5 3 Group 1 2.5 Group 2 2 Group 3 1.5 1 0.5 0 Plasma renin activity Fig. (2): A histogram showing the effect of candisartan treatment on plasma rennin activity ng/m1/h compared to cyclosporine nephrotoxic group 8 60 * 50 40 ** Group 1 30 Group 2 Group 3 20 10 0 Blood urea level mg/dl Fig. (3): A histogram showing the effect of candisartan treatment on blood urea level mg/dl compared to cyclosporine nephrotoxic group 1.6 * 1.4 1.2 1 Group 1 0.8 ** 0.6 Group 2 Group 3 0.4 0.2 0 Serum creatinine mg/dl Fig. (4): A histogram showing the effect of candisartan treatment on serum creatinine mg/dl compared to cyclosporine nephrotoxic group 9 20 18 * 16 14 ** 12 Group 1 10 Group 2 8 Group 3 6 4 2 0 Tissue MDA level Fig. (5): A histogram showing the effect of candisartan treatment on tissue MDA level µM/g compared to cyclosporine nephrotoxic group *significant compared with control normal group. **significant compared with cyclosporine nephrotoxic group. # In significant compared to cyclosporine nephrotoxic group. 10 Fig. (6): A trace showing RBF in control normal rat. Fig. (7): A trace showing RBF in cyclosporine nephrotoxic rat. Fig. (8): A trace showing RBF in candisartan rat. 11 Fig. (9): Cut section of rat kidney of control group showing normal glomeruli and tubules (H& E x100) 12 a b b Fig.(10) a b a b a Fig.(11) Fig. (10&11):Cut section of rat kidney of cyclosporine nephrotoxic group showing cyclosporine induced changes in the form of tubular degeneration (a), vaculation and hyalinosis of the glomerular basement membrane (b) (H& E x40). 13 b a Fig. (12) a b a Fig. (13) Fig. (12&13):Cut section of rat kidney of candisartan treated group showing restoration of the tubular (a) and glomerular (b) structure to a very large extent (H & E x 40). 14 DISCUSSION Cyclosporine is established as the immunosuppressant of choice in human organ transplantation, because it improves graft survival and is not associated with myelosupression. Unfortunately, CsA can lead to a wide spectrum of nephrotoxic complications. Both functional and structural changes in the kidney of transplant patients and experimental animals have been reported (2). The data of the present work revealed that daily administration of CsA 20mg/kg/day S.C for 21 day produced significant reduction of renal blood flow, significant elevation of blood urea and serum creatinine levels. Histopathological examination of renal sections demonstrated that CsA produced tubular atrophy of the proximal convoluted tubules, interstitial fibrosis, hyalinosis of vascular basement membrane and nephrocalcinosis at the corticomedullary junction and calicified concretions in the tubules. These results are in agreement with (11,12) . They reported that, CsA reduce glomerular filtration rate and renal blood flow by causing vasoconstriction of the glomerular afferent arterioles. (13) Reported that cyclosporine decreases renal blood flow by constricting the afferent arteriole proximal to the glomerulus. Also, (1) reported that CsA produced renal vasoconstriction and systemic hypertension. Mean while (14) , reported that CsA causes a dose related decrease in renal function in experimental animals. It produced a significant increase in serum creatinine and blood urea and a significant decrease in creatinine clearance. 15 (1) Reported that in chronic CsA induced nephrotoxicity, the main histological findings in the kidney are the vascular lesions in the endothelium and smooth muscle cells, severe atrophy, vacuolization and thickening of the basal membrane can be found. Moreover, (15) observed that chronic CsA administration leads to loss of proximal tubular epithelial cell integrity and tubular atrophy, a variable interstitial injury with secondary fibrosis. (16) Reported that croticomedullary calcification was seen with CsA. Calcified laminated concretions in tubules and microcalcification of single tubular cells were also seen with CsA. (17) Reported that chronic cyclosporine nephrotoxicity is characterized by interstital fibrosis and afferent arteriolar hyalinosis. In the present work, it was observed that daily oral administration of candisartan 24 hour before and 21 days along with CsA significantly increase renal blood flow, prevented CsA induced elevation in blood urea and serum creatinine. Histopahtological examination of renal sections of candisartan treated group revealed marked improvement as no calcification was detected at all, tubular and hyalinosis of the blood vessels were much less evident. These results are in agreement with(4) who reported that candisartan inhibited the increase in blood urea and serum creatinine induced by CsA. (18) Concluded that candesartan cilexetil can effectively control hypertension and proteinuria without deterioration in renal allograft function. These data suggest that treatment with candesartan cilexetil may be useful for maintaining long-term renal allograft function. 16 (19) Reported that up regulation of vascular endothelial growth factor seem to be related up regulation of angiotensin II in cyclosporine nephrotoxicity. When renal blood flow is substantially reduced, angiotensin II contributes to the maintenance of glomerular filtration rate by constricting the efferent glomerular arterioles. In such condition, dilation of the efferent arterioles by inhibitors of the renin- angiotensin system may potentiate the reduction in glomerular filtration rate. Captopril and saralasin have previously been shown to increase glomerular filtration rate and renal blood flow in CsA treated normotensive rats(20). Enalapril was also able to prevent the CsA- induced decline in glomerular filtration rate in diabetic patients (21). The exact mechanism of CsA-induced nephrotoxicity are not known, but there are several lines of evidence suggesting an involvement of the renin- angiotensin system (4) . This is also supported by our study through the finding that plasma renin activity was higher in the CsAtreated than in the control group. CsA has been reported to stimulate renin production and release in isolated juxtaglomerular cells (22). An increase in plasma renin activity has been demonstrated in CsA-Treated rats either on sodium depletion (3) , on standard chow (23) , or during high intake of sodium (24,25). CsA has also been reported to elevate plasma angiotensin II levels(26). Furthermore,long- term treatment with CsA upregulates AT1 receptors in vascular and renal tissue (27) effect of angiotensin II(28,29). 17 and increases vasoconstrictive Chronic administration of angiotensin II in rats produces renal injury similar to that observed in CsA nephropathy (30,31) Both angiotensin II and CsA cause an overexpression of transforming growth factor (TGF1), a cytokine which has been implicated in the pathophysiology of many fibrotic diseases of the kidney and other organs (31,32) . In addition, tubulointerstitial expression of osteopontin, an adhesion molecule associated with renal fibrosis, is increased by both angiotensin II (30) and CsA(32). Thus, activation of the renin- angiotensin system by CsA may be at least partly responsible for the interstitial fibrosis through stimulation of TGF-1 and osteopontin expression. This is also supported by the finding that the AT1 receptor antagonist losartan reduced the CsAinduced interstitial fibrosis concomitantly with decreased renal TGF-1 and betaig-h3 expression (15). (19) Reported that the increased VEGF expression in chronic CsA nephrotoxicity seems to be related to up-regulation of Ang II. In addition, VEGF probably exerted its effect via the KDR/FLK-1 receptor, the actions of VEGF in this model remain speculative, but may be related to its effect on macrophage infiltration or matrix deposition. The role of reactive oxygen species formation in the CsA induced impairment of renal function has been suggested by(33). (16) Observed that oxygen free radicals are one of different mediators for CsA induced nephrotoxicity. There was increasd production of the lipid peroxidation product malondialdhyde (MDA) with CsA indicating the oxidative stress associated with CsA nephrotoxicity. (34) Reported that melatonin, through its antioxidant properties, significantly antagonized CsA induced renal impairment. 18 (35) Showed that curcumin attenuates cyclosprine induced renal dysfunction and oxidative stress in rat kidneys through its antioxidant properties. (2) Observed that ANG II induce oxidative strees in vitro and in vivo and demonstrated the pivotal role of AT1 receptor bloker (irbisartan) in amelioration of cyclosprine nephrotoxicty through its antioxidant properties. Thus, it is suggested that candisartan produces nephroprotective effect in the rat model of CsA induced nephrotoxicity. This nephroprotection of candisartan is based on a combination of angiotensin receptor antagonism, improvement of endothelial dysfunction and potent antioxidant properties. ACKNOWLEDGMENT Our deep gratitude and appreciation to Dr. Ghada Ahmed Abd El Fattah Lecturer of pathology, Faculty of Medicine, Benha University for her great help and valuable constructive cooperation histospathological part. 19 in the REFERENCES 1- Rodicio, J.L. (2000): Calcium antagonists and renal protection from cyclosporine nephrotoxicity. J. Cardiovasc. Pharmacol. 35 (Suppl. 1): S 7 – S11. 2- Chander V.; Singh D.; Tirkey N.; Chander H. and Chopra K. (2004): Amelioration of cyclosporine nephrotoxicity by irbesartan, A selective AT1 receptor antagonist. nephRen Fail. Sep; 26 (5): 467 – 77. 3- Burdmann E.A. Andoh T.F.; Nast C.C.; Evan A.; Connors B.A.; Coffman T.M.; Lindsley J.; Bennett W.M. (1995): Prevention of experimental cyclosporine-induced instestitial fibrosis by losartan and enalapril. Am. J. Physiol. 269: F491-F499. 4- Padi S.S. and Chopra K. (2002): Selective angiotensin II type I receptor blockade ameliorates cyclosporine nephrotoxicity. Pharmacol Res. May; 45 (5): 413 – 20. 5- Haywood, J.R.; Sahffer, R.A. and FAstenow, C. (1981): Regional blood flow measurement with pulsed Doppler flowmeter in conscious rats. Am. J. Physiol, 242: H273 – H278. 6- Lassila M, Finckenberg P, Pere AK, Krogerus L, Ahonen J, Vapaatalo H and Nurminen ML (2000): Comparison of enalapril and valsartan in cyclosporine A-induced hypertension and nephrotoxicity in spontaneously hypertensive rats on high- sodium diet. Br J Pharmacol. Jul; 130 (6):1339-47. 7- Patton, C.J. and Crouch, S.R. (1977): Blood urea estimation. Anal. Chem. 49, 464. 8- Flavio, V. and William, J.C. (1983): Long term renal function in kidney donors. Transplantation. Vol. 36: No. 6 : P. 626. 9- Aruoma, O.I., Halliwell, B. and Laughton, M.J. (1989): The mechanism of initiation of lipid peroxidation. Evidence against a 20 requirement for an iron (II)-iron (III) complex. Biochemical Journal 258 (2): 617-620. 10- Goldstone, L.A. (1983): Understanding medical statstics. William Heinmann Medical Books Limited, London. (2): 50-52. 11- Araujo LP.; Truzzi R.R.; Mendes GE.; Luz M.A.; Burdmann E.A.; Oliani S.M. (2013): The protective effects of omega 3 fatty acids and sesame oil against cyclosporine A-induced nephrotoxicity. Drug Chem Toxicol. Apr; 39 (2): 241 – 8. 12- Klawitter J.; Bendrick-Peart J.; Rudolph B.; Beckey V.; Klawitter J.; Haschke M.; Rivard C.; Chan L.; Leibfritz D.; Christians U. and Schmitz V. (2011): Urine metabolites reflect time-dependent effects of cyclosporine and sirolimus on rat kidney function. Epub. Nov 19. Chem Res Toxicol. Jan; 22 (1): 118-28. 13- English, J.; Evan, A.; Hoghton, D.C. and Bennett, W.M. (1987): Cyclosporine-induced acute renal dysfunction in the rate: Evidence of arteriorlar vasoconstriction with preservation of tubular function. Transplantation, 44: 135 – 144. 14-Whiting, P.H. and Simpson, J.G. (1988): Lithium clearance measurements as an indicator of cyclosporine A nephrotoxocity in the rat. Clin. Sci., 74: 173 – 178. 15- Sun BK.; Li C.; Lim S.W.; Choi B.S.; Lee SH.; Kim I.S.; Kim Y.S. Bang B.K. and Yang, C.W. (2005): Blockade of angiotensin II with losartan attenuates tansforming growth factor-beta1 inducible gene-h3 (betaig-h3) expression in a model of chronic cyclosporine nephrotoxicity. Nephron ExpNephrol; 99 (1): eg-16. 16- Naidu, M.U.R.; Kumar, K.V.; Shifow, A.A.; Prayag, A. and Ratrakar, K.S. (1999): Lacidipine protects against cyclosporineinduced nephrotoxicity in rats. Nephron, 81: 60 – 66. 17- Shihab F.S.; Yi, H.; Bennett, W.M. and Andoh, T.F. (2000): Effect of nitric oxide modulation of TGF-beta 1 and matrix proteins in 21 chronic cyclosporine nephrotoxicity. Kidney-int. Sep; 58 (3): 1174 – 85. 18- Omoto K.; Tanabe K.; Tokumoto, T.; Shimmura H.; Ishida H. and Toma H. (2003): Use of candesartan cilexetil decreases proteinuria in renal transplant patients with chronic allograft dysfunction. Transplantation. Oct 27; 76 (8): 1170 – 4. 19- Shihab F.S.; Bennett W.M.; Isaac J.; Yi H. and Andoh, T.F. (2002):Angiotensin II regulation of vascular endothelial growth factor and receptors Flt-1 and KDR/FLK-1 in cyclosporine nephrotoxicity. Kidney Int. Aug; 62 (2): 422 – 33. 20- Kaskel F.J.; Devarajan P.; Arbeit L.A.; Partin J.S.; Moore L.C. (1987): Cyclosporine nephrotoxicity: Sodium excretion, autoregulation, and angiotensin II. Am. J. Physiol.; 252: F733-F742. 21- Hannedouche T.P.; Natov S.; Boitard C.; Lacour B.; Grunfeld J.P. (1996): Angiotensin converting enzyme inhibition and chronic cyclosporine-induced renal dysfunction in type 1 diabetes. Nephrol. Dial. Transpant.; 11:673 – 678. 22- Kurtz A.; Della Bruna R.; Kuhn K. (1988): Cyclosporine A enhances renin secretion and production in isolated juxtaglomerular cells. Kidney int.; 33: 947 – 953. 23- Abassi Z.A.; Pieruzzi F.; Nakhoul F.; Kelser H.R. (1996): Effects of cyclosporine A on the synthesis, excretion, and metabolism of endothelin in the rats. Hypertension; 27: 1140 – 1148. 24- Mervaala E.M.A. Pere A.K.; Lindgren L.; Laakso J.; Teravainen TL., Karjala K.; Vapaatalo H.; Ahonen J.; Karppanen H. (1997): Effects of dietary sodium and magnesium on cyclosporine Ainduced hypertension and nephrotoxicity in spontaneously hypertensive rats. Hypertension; 29 : 822 – 827. 25- Mervaala E.M.A.; Lassila M.; Vaskonen T.; Krogerus L.; Lahteenmak T.; Vapaatalo H.; Karppanen H. (1999): Effects of ACE inhibition on cyclosporine A-induced hypertension and 22 nephrotoxicity in spontaneously hypertensive rats on high sodium diet. Blood Pressure.; 8: 49 – 56. 26- Edwards B.D. Chalmers R.J.; O'Driscoll J.B.; Mitchell D.M.; Smith R.J.; Lawson, R.S.; Testa H.J.; Ballardie F.W. (1994): Angiotensin II as a risk factor for cyclosporine nephrotoxcity in patients with psoriasis. Clin. Nephrol.;41 : 350 – 356. 27- Regitz-zagrosek V.; Auch-Schwelk W.; Hess B.; Klein U.; Duske E.; Steffen C. Hilldebr-andt A.G.; Fleck E. (1995): Tissue-and subtype-specific modulation of angiotensin II receptors by chronic treatment with cyclosporine A, angiotensin-converting enzyme inhibitors and AT1 antagonists. J. Cardiovasc. Pharmacol.; 26: 66 – 72. 28-Auch-schwelk W.; Bossaller C.; Gotze S.; Thelen J.; Fleck E. (1993): Endothelin and vascular smooth muscle function after chronic treatment with cyclosporine A.J. Cardiovasc. Pharm. 21: 435-440. 29- Takeda Y.; Miyamori I.; WU P.; Yoneda T.; Furukawa K.; Takeda R. (1995): Effects of endothelin receptor antagonist in rats with cyclosporine-induced hypertension. Hypertension; 26: 932 – 936. 30- Giachelli C.M.; Pichler R.; Lombardi D.; Denhardt D.T.; Alpers C.; Schwarz S.M.; Johnson, R.J. (1994): Osteopontin expression in angiotensin II-Induced tubulointerstitial nephritis. Kidney Int. 45: 515 – 524. 31- Noble N.A.; Border W.A. (1997): Angiotensin II in renal fibrosis: Should TGF-β rather than blood pressure be the therapeutic target. Semin. Nephrol.; 17: 455 – 466. 32- Pichler R.H.; Franceschin N.; Young B.A.; Hugo C.; Andoh T.F.; Burdmann E.A.; Shankland S.J.; Alpers C.E.; Bennett W.M.; Couser W.G.; Johnson R.J. (1995): Pathogenesis of cyclosporine nephropathy: Roles of angiotensin II and osteopontin. J. Am. Soc. Nephrol.; 6: 1186 – 1196. 23 33- Wolf, A.; Clemann, N.; Friehauff, W.; Ryffel, B. and Cordier, A. (1994): Role of reactive oxygen formation in the cyclosporine A medicated impairment of renal functions. Transplant Proc. 16: 2902 – 2907. 34- Kumar, K.V.; Naidu, M.U.; Shifow, A.A.; Prayag, A. and Ratnakar, K.S. (1999): Melatonin an antioxidant protects against cyclosporineinduced nephrotoxicity. Transplantation. Apr. 15; 67 (7): 1065 – 8. 35- Tirkey N.; Kaur, G.; Vij G. and Chopra K. (2005): Curcumin, a diferuloylmethane, attenuates cyclosporine-induced renal dysfunction and oxidative stress in rat kidneys. BMC pharmacol. Oct 15; 5: 15. 24