Breast MRI Screening
advertisement

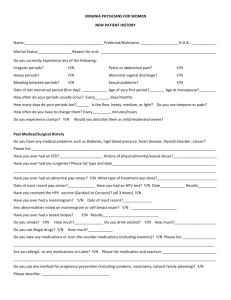
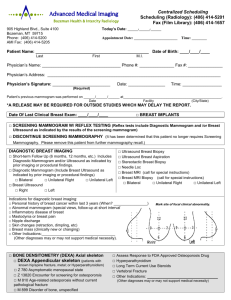
MILFORD HOSPITAL BREAST MRI SCREENING FORM Name______________________________Date of Birth__________________ Weight_______ Date of Last Menstrual Period______________________ Day of Cycle______________________ Any chance of pregnancy?________ Do you have or have you had Breast Cancer? YES _________________When ____________________Where? NO Any other previous surgery on your breasts? ___________________________ Any chemotherapy or radiation therapy? ______________________________ Do you have a family history of Breast Cancer? ________________________________________________________________________ Do you have the BRCA-1 or BRCA-2 gene mutation? YES NO Has anyone in your family tested positive for the BRCA-1 or BRCA-2 gene mutation? YES NO Have you had a recent mammogram? ______________________________ Where? ______________________ Do you have the films? ____________ Any pain and/or lumps in either breast? _______________________RT or LT Any discharge from the nipples? ____________________________ RT or LT Please list all surgeries: Have you ever gotten a piece of metal in your eyes? Have you ever worked as a machinist/welder? Do you have a pacemaker or defibrillator? Do you have a brain aneurysm clip? Any implanted devices in your body? Any cardiac stents? Do you have: ____ DIABETES YES YES YES YES YES YES NO NO NO NO NO NO _____KIDNEY DISEASE _____RENAL FAILURE I ATTEST THAT THE ABOVE INFORMATION IS TRUE TO THE BEST OF MY KNOWLEDGE. I HAVE READ AND UNDERSTAND THE ENTIRE CONTENTS OF THIS FORM AND HAD THE OPPORTUNITY TO ASK QUESTIONS REGARDING THIS INFORMATION. SIGNATURE __________________________________DATE_______________ TECHNOLOGIST SIGNATURE_______________________DATE___________