PNEUMONIA – INVESTIGATION AND MANAGEMENT GUIDELINES
advertisement

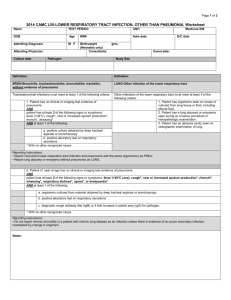
Paediatric Protocol Respiratory: 3.5 September 2004 PNEUMONIA – INVESTIGATION AND MANAGEMENT GUIDELINES First distributed 1996- Revised Sept 2000 (Helena Clements), September 2004 (Maria Atkinson). Background This guideline is based on the following 3 documents: 1. Evidence Based Guideline – Management of Community Acquired Pneumonia in Children drawn up by the British Thoracic Society (BTS) 2002 [1]. 2. A Prospective Study of the Aetiology of Community Acquired Pneumonia completed in Nottingham in 1997 [2]. The Nottingham study showed that in 89 children a diagnosis was achieved in 48. Seven children had Streptococcus pneumoniae, 14 had Mycoplasma, 6 had Pertussis and 1 had Chlamydia. Twenty-three children had a viral cause of which respiratory syncytial virus (RSV) was commonest. Three children had dual infections. Chest radiographs and acute phase reactants did not help distinguish between different bacterial and viral aetiologies. This study led to use of benzyl penicillin as first line antibiotic treatment in children with pneumonia. 3. A Multicentre RCT Comparing Oral Amoxicillin and IV Benzyl penicillin for Community Acquired Pneumonia (CAP) PIVOT Trial (submitted for publication). Lead centre Nottingham, completed June 2004. This study involving over 250 children from 8 different centres demonstrated that oral and IV treatment are equivalent for CAP in previously well children who were unwell enough to require admission to hospital. Complications such as empyema were not increased in the oral arm. Time to resolution of symptoms was the same in both groups (median 9 days). CLINICAL PRESENTATION Some features such as wheeze and hyperinflation on CXR make a diagnosis of viral pneumonia more likely. However, studies have consistently shown [3] that it is not possible to distinguish viral and bacterial pneumonia by presenting symptoms, signs or radiological changes. Therefore, all children with pneumonia should be treated with antibiotics. Clinical presentation varies, pneumonia can sometimes be difficult to diagnose. Many children present with classical symptoms such as cough, difficulty breathing, fever and tachynoea. However some children with pneumonia have a normal respiratory rate and clear chest. It should be remembered that pneumonia is a differential for PUO and can also present with referred pain to the abdomen. If you are faced with a child with breathing difficulty and are unsure whether they have pneumonia or another respiratory disorder please refer to the “Nottingham Evidence Based Guideline on Management of Breathing Difficulty in Children”. Author: Dr Maria Atkinson 1 Does the child need admission to hospital ? Any child with 1 or more of the features below should be admitted to hospital for further management Infants SaO2 <92%, cyanosis RR> 70/min Difficulty breathing Intermittent apnoea, grunting Not feeding Family not able to provide appropriate observation or supervision Older Children SaO2 <92%, cyanosis RR >50/min Difficulty breathing Grunting Signs of dehydration Family not able to provide appropriate observation or supervision Admission required? No Yes Are any of the following features present ? Oxygen saturations <85% air Still shocked following 20mls/kg fluid resuscitation Chronic lung disease such as cystic fibrosis Definite penicillin allergy Large pleural effusion Established diagnosis of immunodeficiency < 6 months Management Investigations – CXR is not necessary to confirm the diagnosis in children with mild disease well enough to be discharged home [4]. Blood tests are not indicated. Discharge with a 7 day course of amoxicillin (doses from Medicines For Children). Calpol and ibuprofen for pain relief and temperature control Advise the parents to seek further medical attention if the temperatures are not settling in 48 hours, the child is unable to tolerate oral antibiotics or they become more unwell. See page 3 Author: Dr Maria Atkinson 2 No Yes Treat with oral amoxicillin, erythromycin if penicillin allergic (doses Medicines Children) CXR NO indication for FBC, CRP, B/C or serology NPA or viral throat swab for viral immunofluoresence and culture Treat with IV antibiotics see Table below (doses Medicines Children) CXR FBC, CRP, B/C, serology (1-2mls clotted blood for respiratory pathogens) NPA or viral throat swab for viral immunofluoresence and culture General inpatient Care Adequate fluid intake orally, NG or IV fluids at 80% maintenance (watch for SIADH). Oxygen to keep saturations >92% Chest physiotherapy is not beneficial Antipyretics and analgesics Choice of antibiotic in those requiring IV treatment < 6 months Cefuroxime Pathogens include gram negatives e.g. E. coli and gram positives e.g. Group B Streptococci therefore a broad spectrum antibiotic is needed until culture and sensitivities are known. Also consider pertussis > 6 months Benzyl penicillin Clarithromycin if penicillin allergic Aspiration pneumonia Metronidazole + Benzyl penicillin. Usually suggested by history. ‘At risk’ groups are children with neurological problems such as cerebral palsy, or acute problems such as febrile convulsions or head injury. Need to cover anaerobic organisms. Coexisting disease such as cystic fibrosis, Refer to appropriate protocol or discuss immunodeficiency, oncology patients. with microbiology if unsure All doses should be taken from Medicines For Children Author: Dr Maria Atkinson 3 Failure to respond to first line treatment The majority of children with pneumonia will respond to treatment within 48 hours. If the child remains unwell with high temperatures at 48 hours consider the following. 1. Mycoplasma pneumoniae infection Historically this was thought to be far more common in older children but it is increasing being recognised as a cause of pneumonia in the < 5 year age group [5, 6]. It may present with patchy infiltrates or consolidation on the CXR. Add erythromycin (PO) or clarithromycin IV if oral medication not tolerated. 2. Empyema Repeat CXR. If pleural effusion or empyema is present discuss with the paediatric surgical registrar on call. Further imaging such as chest USS may be indicated prior to surgery or drainage. 3. Antibiotic cover If addition of a macrolide fails to confer improvement, consider a change to a broader spectrum antibiotic such as cefuroxime IV, examine for empyema and repeat CXR. 4. Rare causes to consider – lung abscess, coexisting disease that may be undiagnosed such as immunodeficiency. 5. Take blood for FBC, CRP, B/C and acute serology for respiratory pathogens if not already sent. Follow Up Outpatient follow up – not routine if complicated, prolonged recovery (i.e. more than 5 days in hospital) or empyema if parents call re. continuing concerns or child has continuing symptoms or GP prescribes repeat course of antibiotics Follow up CXR’s are only indicated in the following situations (7). Lobar collapse or in a child with persistent symptoms. Author: Dr Maria Atkinson 4 1. 2. 3. 4. 5. 6. 7. Guidelines For Treatment of Community Acquired Pneumonia In Children. 2002, British Thoracic Society. Clements, H., et al., Rationalised prescribing for community acquired pneumonia: a closed loop audit. Archives of Disease in Childhood, 2000. 83: p. 320-324. Virkki, R., et al., Differentiation of bacterial and viral pneumonia in children. Thorax, 2002. 57(57): p. 428-441. Swingler, G. and M. Zwarenstein, Chest radiograph in acute respiratory infections in children. Cochrane Database Systematic Reviews, 2000. 2. Harris, J., et al., Safety and efficacy of azithromycin in the treatment of community-acquired pneumonia in children. The Pediatric Infectious Disease Journal, 1998. 17(10): p. 865-871. Eposito, S., et al., Mycoplasma pneumoniae and Chlamydia pneumoniae infections in children with pneumonia. Europea Respiratory Journal, 2001. 17: p. 241-254. Gibson N, Hollman A, Paton J BMJ 307 1117 1993 Value of radiological FU of childhood pneumonia) Author: Dr Maria Atkinson 5