Table 3 - Springer Static Content Server
advertisement

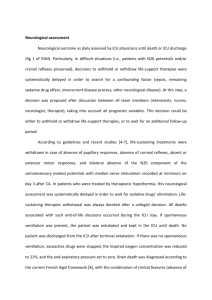
Electronic supplementary data. Intensive care unit mortality after cardiac arrest: the relative contribution of shock and brain injury in a large cohort. Virginie Lemiale, MD(1,5) ; Florence Dumas, MD(2,6); Nicolas Mongardon, MD(1,5) ; Olivier Giovanetti, MD(6) ; Julien Charpentier,MD(1,5); Jean-Daniel Chiche, MD(1,5) ; Pierre Carli, MD(4,5) ; Jean-Paul Mira, MD(1,5) ; Jerry Nolan, FRCA, FRCP(3) ; Alain Cariou, MD(1,5,6) 1 Medical Intensive Care Unit, Cochin Hospital, Groupe Hospitalier Universitaire Cochin Broca Hôtel-Dieu, Assistance Publique des Hôpitaux de Paris, 27 rue du Faubourg SaintJacques, 75014 Paris, France 2 Emergency Department, Cochin Hospital, Groupe Hospitalier Universitaire Cochin Broca Hôtel-Dieu, Assistance Publique des Hôpitaux de Paris, 27 rue du Faubourg Saint-Jacques, 75014 Paris, France 3 Intensive Care Unit, Royal United Hospital, Combe Park, BA1 3NG, Bath, United- Kingdom 4 SAMU 75, Necker Hospital, Assistance Publique des Hôpitaux de Paris, 149, rue de Sèvres,- 75015Paris, France 5 Université Paris Descartes, Sorbonne Paris Cité, Faculté de Médecine, 15 rue de l’Ecole de Médecine, 75006 Paris, France 6 INSERM U970, Paris Cardiovascular Research Center (PARCC), European Georges Pompidou Hospital, 56 rue Leblanc, 75015 Paris, France Management of OHCA patients during ICU stay Briefly, since 2000, immediately after OHCA and when no obviously other etiology than cardiac origin was retained, all patient had coronary angiogram with PCI if needed. When coronary angiography was not conclusive, brain and angio-thoracic CT scan were performed. When indicated, hypothermia treatment was initiated immediately at ICU admission using external cooling by forced cold air during the first 24 hours to obtain a target temperature between 32 and 34°C as recommended by international guidelines [1,2]. During the first 48 hours of ICU stay, treatments were adapted to maintain homeostasis with glucose control, normocapnia maintenance, inspired fraction of O2 (FiO2) for arterial saturation of 94-98%, mean arterial pressure target as 65-70mmHg, and hemoglobin level over 7g/dL [3]. Neurological assessment Neurological outcome as daily assessed by ICU physicians until death or ICU discharge (fig 1 of ESM). Particularly, in difficult situations (i.e., patients with N20 potentials and/or cranial reflexes preserved), decisions to withhold or withdraw life-support therapies were systematically delayed in order to search for a confounding factor (sepsis, remaining sedative drug effect, intercurrent disease process, other neurological disease). At this step, a decision was proposed after discussion between all team members (intensivists, nurses, neurologist, therapist), taking into account all prognostic variables. This decision could be either to withhold or withdraw life-support therapies, or to wait for an additional follow-up period. According to guidelines and recent studies [4-7], life-sustaining treatments were withdrawn in case of absence of pupillary responses, absence of corneal reflexes, absent or extensor motor responses, and bilateral absence of the N20 component of the somatosensory evoked potentials with median nerve stimulation recorded at minimum on day 3 after CA. In patients who were treated by therapeutic hypothermia, this neurological assessment was systematically delayed in order to wait for sedative drugs’ elimination. Lifesustaining therapies withdrawal was always decided after a collegial decision. All deaths associated with such end-of-life decisions occurred during the ICU stay. If spontaneous ventilation was present, the patient was extubated and kept in the ICU until death. No patient was discharged from the ICU after terminal extubation. If there was no spontaneous ventilation, vasoactive drugs were stopped, the inspired oxygen concentration was reduced to 21%, and the end-expiratory pressure set to zero. Brain death was diagnosed according to the current French legal framework [8], with the combination of clinical features (absence of motor response, spontaneous ventilation and brainstem reflex) and the absence of electroencephalographic activity or cerebral perfusion during cerebral CT scan. References 1. 2. 3. 4. 5. 6. 7. 8. 9. Cummins RO, Chamberlain DA, Abramson NS, Allen M, Baskett PJ, Becker L, Bossaert L, Delooz HH, Dick WF, Eisenberg MS, et al. (1991) Recommended guidelines for uniform reporting of data from out-of-hospital cardiac arrest: the Utstein Style. A statement for health professionals from a task force of the American Heart Association, the European Resuscitation Council, the Heart and Stroke Foundation of Canada, and the Australian Resuscitation Council. Circulation. 84:960-75. Nolan JP, Morley PT, Vanden Hoek TL, Hickey RW, Kloeck WG, Billi J, Böttiger BW, Morley PT, Nolan JP, Okada K, Reyes C, Shuster M, Steen PA, Weil MH, Wenzel V, Hickey RW, Carli P, Vanden Hoek TL, Atkins D; International Liaison Committee on Resuscitation. (2003) Therapeutic hypothermia after cardiac arrest: an advisory statement by the advanced life support task force of the International Liaison Committee on Resuscitation. Circulation. 108:118-21. Neumar RW, Nolan JP, Adrie C, Aibiki M, Berg RA, Böttiger BW, Callaway C, Clark RS, Geocadin RG, Jauch EC, Kern KB, Laurent I, Longstreth WT Jr, Merchant RM, Morley P, Morrison LJ, Nadkarni V, Peberdy MA, Rivers EP, Rodriguez-Nunez A, Sellke FW, Spaulding C, Sunde K, Vanden Hoek T. (2008) Post-cardiac arrest syndrome: epidemiology, pathophysiology, treatment, and prognostication. A consensus statement from the International Liaison Committee on Resuscitation (American Heart Association, Australian and New Zealand Council on Resuscitation, European Resuscitation Council, Heart and Stroke Foundation of Canada, InterAmerican Heart Foundation, Resuscitation Council of Asia, and the Resuscitation Council of Southern Africa); the American Heart Association Emergency Cardiovascular Care Committee; the Council on Cardiovascular Surgery and Anesthesia; the Council on Cardiopulmonary, Perioperative, and Critical Care; the Council on Clinical Cardiology; and the Stroke Council. Circulation. 118:2452-83. Morley PT, Atkins DL, Billi JE, Bossaert L, Callaway CW, de Caen AR, Deakin CD, Eigel B, Hazinski MF, Hickey RW, Jacobs I, Kleinman ME, Koster RW, Mancini ME, Montgomery WH, Morrison LJ, Nadkarni VM, Nolan JP, O'Connor RE, Perlman JM, Sayre MR, Semenko TI, Shuster M, Soar J, Wyllie J, Zideman D. (2010) Part 3: Evidence evaluation process: International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation. 122:S283-90. Peberdy MA, Callaway CW, Neumar RW, Geocadin RG, Zimmerman JL, Donnino M, Gabrielli A, Silvers SM, Zaritsky AL, Merchant R, Vanden Hoek TL, Kronick SL. (2010) Part 9: post-cardiac arrest care: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 122:S768-86 Wijdicks EF, Hijdra A, Young GB, Bassetti CL, Wiebe S. (2006) Quality Standards Subcommittee of the American Academy of Neurology. Practice parameter: prediction of outcome in comatose survivors after cardiopulmonary resuscitation (an evidence-based review): report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology. 67:203-10. Booth CM, Boone RH, Tomlinson G, Detsky AS. (2004) Is this patient dead, vegetative, or severely neurologically impaired? Assessing outcome for comatose survivors of cardiac arrest. JAMA. 291:870-9. [No authors listed] (1968) A definition of irreversible coma. Report of the Ad Hoc Committee of the Harvard Medical School to Examine the Definition of Brain Death. JAMA. 205: 337-40. Décret no 96-1041 du 2 décembre 1996 (1996) relatif au constat de la mort préalable au prélèvement d'organes, de tissus et de cellules à des fins thérapeutiques ou scientifiques et modifiant le code de la santé publique (deuxième partie : Décrets en Conseil d'Etat). JORF 282 : 17615 Figure 1 ESM : decision algorithm for post-CA patients. EEG: electro-encephalogram; ICU: Intensive Care Unit. Figure 2 ESM : Mode of death according to the study period Table 1 ESM: Baseline characteristics according to the mode of death Total n=1152 ICU survival n=384 57 (16) 294 (76) 203 (54) ICU death related to post cardiac arrest shock n=269 61 (16) 191 (71) 103 (39) ICU death related to neurological injury n=499 59 (16) 357 (71) 158 (32) Age, yrs (SD) Male sex, n(%) Bystander CPR, n(%) Cardiac arrest location, n(%) Home Public area 59 (16) 842 (73) 464 (41) 771 (67) 378 (33) 212 (55) 172 (45) 192 (72) 74 (28) 367 (74) 132 (26) Shockable rhythm, n(%) 654 (57) 294 (77) 124 (46) 236 (47) Time from collapse to ROSC <12 min 12-20 min 20-31 min > 31min 252 (25) 205 (20) 292 (29) 257 (26) 150 (44) 88 (26) 63 (18) 41 (12) 32 (15) 32 (15) 66 (30) 88 (40) 70 (16) 85 (19) 163 (37) 128 (29) Admission lactate value <2.5 mmol/l 2.5-5 mmol/l 5-9.3 mmol/l >9.3 mmol/l 247 (26) 240 (25) 238 (25) 242 (25) 161 (49) 88 (26) 56 (17) 21 (6) 13 (6) 25 (12) 40 (19) 132 (63) 73 (17) 127 (29) 142 (33) 89 (21) 294 (26) 265 (24) 281 (25) 276 (25) 165 (43) 94 (25) 71 (19) 53 (14) 212 (55) 272 (71) - 22 (9) 37 (15) 76 (32) 106 (44) 269 (100) 136 (50) 2 (1-3) 107 (22) 134 (27) 134 (27) 117 (24) 308 (62) 356 (71) 8 (5-10) Admission creatinine value <92 mol/l 92-115 mol/l 116-149 mol/l > 150 mol/l Post CA shock, n(%) Therapeutic hypothermia, n(%) Delay between CA and ICU death, days, median (IQR) 789 (68) 764 (66) 5 (2-9) % are taking into account missing data SD=Standard deviation CPR= Cardiopulmonary Resuscitation VF/VT=Ventricular Fibrillation/Ventricular Tachycardia ROSC= Restoration of Spontaneous Circulation OHCA=Out-of Hospital Cardiac Arrest ICU=Intensive Care Unit IQR= Interquartile (p25-p75) p-value 0.001 0.169 <0.001 <0.001 <0.001 <0.001 <0.001 <0.001 <0.001 <0.001 0.001 Table 2 ESM Multivariate analysis according to mode of death (result from multiples imputations). Imputated variables: location (n=3), bystander CPR (n=22), creatinine level (n=36), lactate level (n=185), time to ROSC (n=146) Deaths related to post cardiac arrest shock n=269 Deaths related to neurological injury n=499 OR Ratio (95% CI) OR (95% CI) p-value Age, yrs 1.02 [1.01-1.04] 0.001 1.01 [1.0-1.02] 0.047 Male gender, n(%) 0.83 [0.51-1.34] 0.93 0.89[0.61-1.30] 0.55 CPR by bystander, n(%) 0.70 [0.45-1.09] 0.12 0.56 [0.41-0.78] 0.001 Cardiac arrest Location, n(%) (home vs public area) 0.68 [0.44-1.06] 0.09 0.59 [0.42-0.83] 0.002 Shockable rhythm, n(%) 0.40 [0.25-0.61] <0.001 0.32 [0.22-0.45] <0.001 Time from Collapse to ROSC 1.88[1.47-2.40] <0.001 1.76 [1.49-2.07] <0.001 Admission lactate 2.58 [1.98-3.36] <0.001 1.58[1.33-1.88] <0.001 Admission creatinine 1.55[1.25-1.92] <0.001 1.20[1.03-1.41] 0.02 Post-CA shock, n(%) - - 0.85 [0.61-1.19] 0.35 0.35 [0.23-0.54] <0.001 1.04 [0.74-1.47] 0.82 Therapeutic hypothermia, n(%) OR= Odds Ratio * reference value is survivors (n=386) CPR= Cardiopulmonary Resuscitation VF/VT=Ventricular Fibrillation/Ventricular Tachycardia ROSC= Restoration of Spontaneous Circulation OHCA=Out-of Hospital Cardiac Arrest p-value