Renal Cancers
advertisement

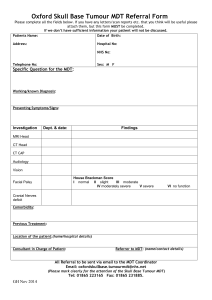
RENAL CANCER MDT DIRECT REFERRAL FORM TO LTHT Date of MDT: Name of referring consultant: Hospital: Please select your hospital Patient Details/ Addressograph: Surname: First Name: Date of Birth: Address: NHS Number: Patient Contact Number: GP. Name: GP Phone No: Family history of renal cancer Yes No History of diabetes Yes No History of hypertension Yes No History of any renal disease Yes No History of renal surgery Yes No Symptoms – loin pain Yes No Symptoms – haematuria Yes No Symptoms – incidental Yes No Any other co-morbidities Examination findings U&E Cr eGFR Ca LFT Patient’s wishes Imaging to be sent (to be reviewed in specialist MDT): Yes If YES Ultrasound CT Chest X-ray MRI DMSA Bone scan No MDT provisional plan: Surgery Curative intent Diagnostic surgical procedure only Oncology BSC Comment: 62 Day Breach Date: Key Worker/CNS Name: Details of Person Competing Form: Name: Role: Date: Attach this electronic form to the PPM documents tab Version 1 (Wednesday, 14 December 2011)