Autumn 2002 - The Scottish Renal Registry

Quantitative morphometric analysis of Lupus Nephritis reveals the prognostic significance of interstitial infiltrate, tubular atrophy, but not scarring
Hunter M, Bellamy C, Duffield JS
MRC Centre for Inflammation Research, Department of Pathology, Medical School,
University of Edinburgh
The WHO Criteria for Lupus nephritis have proved useful in predicting progression in those with Class IV disease. However, for those with class III or V disease the predictive power of the criteria is less clear. Further, some patients with class IV nephritis have benign disease. Decisions based solely on these criteria are weighty since they involve cytotoxic therapy in young patients. Because of the obvious deficiencies in current histological criteria and associated interstitial disease in lupus nephritis, other subjective criteria have been assessed such as activity and chronicity indices. The predictive power has proved variable. With the advent of digital image technology we have devised four economical, quick, but robust, reproducible and entirely objective assays for assessing polymeric collagen, collagenous matrix, inflammatory infiltrate and tubular space in whole biopsies. First renal biopsies and data were collected retrospectively on all patients with Lupus presenting to a single nephrology centre over 15 years. The biopsy-derived data and clinical outcomes were compared.
Increased tubular space predicated doubling of creatinine with time (P<0.01), moderate and severe relapse, and death from a renal cause (P<0.01, P<0.05, P<0.01 respectively). The density of nuclei on the whole biopsy, in addition to significantly correlating with initial creatinine clearance, initial proteinuria and initial plasma albumin, also predicted outcome (doubling of creatinine (P<0.05), ESRF (P<0.01). Collagen matrix did not correlate with parameters at the time of the biopsy nor did it predict outcome. Although fibrillary collagen predicted doubling of creatinine (P<0.05), it did not correlate with any other markers of progression/poor outcome.
This new approach to analysis of lupus nephritis is economical and robust. We have validated the assays for a cohort of patients with lupus nephritis. Inflammatory infiltrate and tubular atrophy were confirmed as important predictors of outcome. Interestingly the amount of scarring seen on biopsies did not correlate well with outcome. Given the known deficiencies of the WHO criteria, we believe these assays should be applied to a prospective study as an adjunct to guiding therapy and prognosticating.
Validation of the Cockcroft-Gault equation in the Tayside population
I MacLeod, J Davidson*, IS Henderson and A Severn
Renal Unit and *Dept of Nuclear Medicine, Ninewells Hospital,
Dundee
The Cockcroft-Gault equation is widely used as an estimate of creatinine clearance. To evaluate its accuracy in our population, we compared GFR, measured by 51 Cr-EDTA clearance, with estimated creatinine clearance in 50 patients.
GFR and serum creatinine concentration were measured in 27 women and 23 men, who were attending renal clinics. The age range was 19-89years, weight range 50.1-129.5kg, and measured GFR 14.6-205.3ml/min.
For the whole group, the correlation coefficient was 0.77. The slope was 0.95 and intercept 14.99. Agreement between estimated creatinine clearance and measured GFR was better in women (correlation coefficient 0.8; slope 0.98; intercept 9.78) than in men (correlation coefficient 0.62; slope 0.77; intercept
36.8). Agreement was better in those with poorer renal function; in those with estimated creatinine clearance <80ml/min, correlation coefficient was 0.78, slope
1.4 and intercept –14.46; in those with estimated creatinine clearance >80ml/min, correlation coefficient was 0.44, slope 0.59 and intercept 54.5.
More women than men had estimated creatinine clearances of less than
80ml/min (18 v 5).
The Cockcroft-Gault equation reliably estimates creatinine clearance in patients with impaired renal function.
Kidney Donor Organs: Glasgow 1972-1984
John Crawford and David Hamilton
Departments of Anaesthesia and Transplantation
Western Infirmary, Glasgow.
Criteria for 'brain death' were first proposed by the Harvard 'ad hoc' Committee in 1968, and after finding a role in intensive care practice, revised guide lines on brain stem death (BSD) were approved, among others, by the Royal Colleges in Britain in 1976.
The data recorded on all kidneys obtained and used in Glasgow in the period 1972-1984 were reviewed. Of many changes in this period, the most marked was a reduction in warm times, i.e. the time between cessation of normal blood perfusion and cooling of the organ. The decline and abolition of warm time was related to the rise in use of BSD in clinical practice.
These data shows that use of BSD donation was slow to enter routine transplantation practice and that zero warm times only became common in the mid-1980s. Until then there was a variety of procedures still in use in elective donation, including non-heart beating (cardiac death) and non-ventilated heartbeating donation, with or without early or delayed use of aortic perfusion.
This study shows that the advantages offered to transplantation by the acceptance of BSD in clinical practice were not taken up immediately but were instead acceepted cautiously and incrementally in organ transplantation , particularly kidney transplantation, many years after the official relevant guide lines appeared.
Improved renal transplant outcome in the modern era
N. Padmanabhan, R Sriraman, Y.M. Woo, A.G. Jardine, A E Aulmann and C.C. Geddes:
Renal Unit, Western Infirmary, Glasgow
Introduction In recent years the management of renal transplants has been transformed by the advent of new immunosuppressive agents, organ sharing networks and, possibly, the use of more “marginal” donors. The aim of this study was to assess the impact of these changes on the outcome of transplants performed in a single centre. We compared
3 year patient and graft survival of first cadaveric adult transplants performed in two eras:
1985-1994, when immunosuppression was based on Cyclosporin, Azathioprine and
Prednisolone (Cohort 1, n=575); and 1997-2000, when several other immunosuppressive agents were in use and the present UK Transplant matching scheme had become established (Cohort2, n=237).
Results Median follow up in Cohort 1 was 7.22 years and in Cohort 2 was 3.05 years. In cohort 2 recipients spent longer on the transplant waiting list (922 v 546 days, p<0.0001), donor age was higher (43.1 v 37.1 years, p<0.001) and the incidence of acute rejection was lower (27.8 v 43.5%, P,0.001). In cohort 2, although the proportion of patients receiving a 000 mismatch fell slightly (10.9 v 6.8%, p<0.001), the proportion of transplants with a favourable mismatch was higher (52.7 v 30.4%, p<0.001). There were no significant differences in recipient age, gender, the proportion of recipients with diabetic nephropathy or incidence of delayed graft function. 3 year actuarial graft survival and graft survival censored for patient death were higher in cohort 2 &97% v
67.7%, p 0.0003 and 83.6% v 73.2%, p 0.001, respectively). There was a trend to improved patient survival in cohort 2 that did not reach significance. By multivariate analysis, transplantation in cohort 2 was independently associated with a reduced risk of patient death (Hazard ration [HR] 0.49, p=]0.016) and reduced overall graft failure (HR
0.59, p=0.0.016), but was only associated with reduced graft survival censored for patient death if acute rejection was excluded from the model (HR0.58, p=0.026).
Conclusion Transplantation in the modern era is associated with a significant improvement in graft survival, which is directly related to a reduction in acute rejection.
Patient survival has also improved and we speculate that this may be due to several factors, including improvements in immunosuppressive protocols and advances in the management of cardiovascular disease and infection.
Tacrolimus pharmacogenetics: polymorphisms associated with expression of cytochrome P4503A5 and P-glycoprotein correlate with dose-requirement
Iain A.M. Macphee 1 , Salim Fredericks 2 , Tracy Tai 2 , Petros Syrris 3 , Nicholas D. Carter 3 , Atholl Johnston 4 ,
Lawrence Goldberg 5 , David W. Holt 2 .
1 Division of Renal Medicine, 2 Analytical Unit, 3 Medical Genetics, St. George’s Hospital Medical School,
London. 4 Clinical Pharmacology, Barts and the London, School of Medicine, London. 5 Renal Medicine,
Royal Sussex County Hospital, Brighton.
There is marked heterogeneity in blood concentrations of tacrolimus following standard body weight-based dosing. This is most apparent in Black patients, who have a higher dose-requirement when compared to other ethnic groups. Differences in intestinal P-glycoprotein and hepatic and intestinal cytochrome
P4503A (CYP3A) activity have been postulated as contributing to this problem.
The dose-normalised blood concentrations of tacrolimus at 3 months after renal transplantation were related to single nucleotide polymorphisms (SNP) in the CYP3AP1 pseudogene (A/G-
44
), that previously has been noted to be commoner in African Americans and strongly associated with hepatic CYP3A5 activity, and the C3435T SNP in the MDR-1 gene which influences intestinal P-glycoprotein expression.
The CYP3AP1 genotype correlated well with the tacrolimus dose -requirement. A weaker association was found for the MDR-1 genotype (Table). A significantly higher proportion of individuals possessing a Gallele at the CYP3AP1 (A/G-
44
) SNP failed to reach target blood tacrolimus concentrations during the first week after transplantation than AA homozygotes (39.6% vs 8.8%, p<0.0001).
Single nucleotide polymorphism
Genotype Tacrolimus blood concentration
(No. of patients) per 0.1 mg/kg dose
(Median, inter-quartile range) p vs AA or TT
(Mann-Whitney)
CYP3AP1 (A/G-
44
) AA (126)
AG (45)
GG (9)
MDR-1 (C3435T) TT (62)
CT (70)
CC (48)
9.2 (6.4-13.7)
5.1 (3.5-6.9)
4.2 (2.4-7.1)
9.3 (6.3-14.6)
7.6 (5.1-10.7)
6.3 (4.7-8.7)
-
<0.0001
0.001
-
0.04
0.002
Conclusions
The CYP3AP1 genotype is a major factor in determining the dose-requirement for tacrolimus, and genotyping may be of value in planning patient-specific drug-dosing.
Investigation of an unusual crystal tubulopathy.
Kinga Musial, Christopher Bellamy, Juan Zou, Nick Sargeant and Neil Turner.
Renal Medicine, Royal Infirmary of Edinburgh
Immunoglobulin light chains can cause renal damage in at least five different ways. Firstly, their presence may be associated with multiple myeloma, resulting in cast nephropathy, which is identified by the presence of proteinaceous casts in the renal tubules. Secondly, light chain deposition disease may cause glomerulopathy. Other, less frequent, manifestations of light chain renal accumulation include amyloidosis, hypercalcaemia and fibrillary nephritis.
Here we report an unusual case of crystal tubulopathy observed in a 48 year old man, who presented with tiredness and polyuria. Clinical examination was normal. Serum creatinine was 210
mol/l, having been normal 2 years previous, and other blood results were within the normal range. 24-hour urinary protein excretion was 1g, urine sediment unremarkable. Renal biopsy showed crystal-containing proximal tubular cells. An extensive search for causes of crystalluria was negative. Examination of urine pellet revealed some crystals similar to those found in tubular cells. Subsequently immunofixation identified free kappa chains in the urine. A sensitive light chain assay revealed the presence of free kappa chains in blood at 205mg/l (normal range 3.6-
16mg/l). Serum immunoglobulins, protein electrophoresis and bone marrow examination were normal.
Occasional literature reports describe rare cases of adult Fanconi syndrome secondary to light chain gammopathy, presenting with crystal deposits in renal tubular cells. However, patients have usually had myeloma or other clinical manifestations resulting from light chain deposition. Our patient had no such signs or, indeed, many signs of proximal tubule transport impairment. To our knowledge, this is the first report of such crystal deposition in tubular cells coexisting with inconclusive clinical history.
Further investigations to establish chemical and physical characteristics of the light chain will be presented.
Donor Glomerular Sclerosis has Significant Impact on Function and Survival of Cadaveric Renal Transplants.
ILHAM MA.
1 , BAGUL A.
1 , GRIFFITHS D.
2 , JUREWICZ WA.
2 , OSMAN H.
1
Western Infirmary, Glasgow.
1 , University Hospital of Wales, Cardiff, 2
In the quest to expand transplantation an increasing number of kidneys are retrieved from “marginal” donors. This calls for the need to develop algorithms to assess the quality of grafts prior to allocation.
Aim
To determine if the percentage of donor glomerular sclerosis accurately reflects the “quality” of an organ and has an impact on graft function and survival.
Material & Methods
All cadaveric renal transplants on calcineurin-inhibitor triple therapy with an adequate renal wedge biopsy at the time of transplant were included. Total numbers of normal and globally sclerosed (GS) glomeruli were assessed and reported as a percentage of sclerosed glomeruli (PSG). Clinical donor and recipient data was obtained from the core data forms, case notes and computer network proton system.
Results
Two hundred and thirty patients satisfied inclusion criteria. There were 138 grafts without sclerosed glomeruli (PSG = 0% -
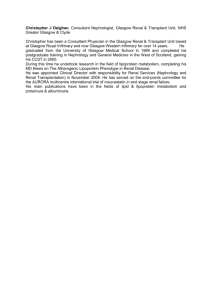
Group1) and 92 kidneys (40%) showed glomerular sclerosis ranging from 1% to 60%. Patients with PGS>0% were divided into 3 groups. Group 2 represented PGS of up to 10% (n=48), Group 3 PGS 10%-20% (n=24) and Group 4 PGS>20% (n=20). The GFR for each of the 4 groups is shown in Figure 1. The median observation period was 3.8 years (range 1.0 - 6.3 years). Grafts with sclerosed glomeruli demonstrated inferior renal function as early as 3 rd post-operative day (median GFR 16ml/min vs. 24ml/min; p<0.001, Mann Whitney test) and a significant difference persisted throughout the observation period (median GFR at 1 and 4 years was 49ml/min vs. 62ml/min; p<0.001 and 31ml/min vs. 51ml/min; p=0.01 respectively).
96
81
66
51
36
21
6
Group 1 ( PGS = 0)(n=129)
Group 2 (PGS 0.1-10%)(n=42)
Group 3 (PGS 10.1-20%)(n=22)
Group 4 (PGS > 20%)(n=17) p value*
Donor Day 0 Day 3 Day 7 Day 90 Day 180 1 year 2 years 3 years 4years
97
91
85
75
0.028
9
9
9
8
1
24
24
19
13
36
42
32
16
60
47
46
38
0.015
0.002
0.000
64
51
49
39
0.000
62
55
51
36
60
50
41
27
55
42
45
24
0.000
0.000
0.008
51
34
30
7
0.018
Figure 1. Median renal function of donors (DGFR) and subsequent GFR of recipients at time zero (GFR0), on 3rd post-op day (GFR3D), at 1 week
(GFR1W), at 3 and 6 months (GFR3M and GFR6M) and at 1,2,3 and 4 years (GFR1,2,3,and GFR4) in 4 groups of patients depending on PGS at time zero
Based on median GFR between year 1 and 4 linear trends were extended to predict function at 10 years. Patients without glomerular sclerosis had the highest GFR at 1 year (66.5 ml/min) and the slowest deterioration (-3.8 ml/min/year). In contrast, patients with PGS>20% had the lowest GFR at 1 year (46.0 ml/min) and the steepest rate of annual deterioration (-9.0 m/min/year)
.
The PGS had a significant effect on transplant survival. Actuarial 5-year Kaplan Meier graft survival for the four groups was 80%,
88%, 59% and 35% respectively (p=0.04, Log Rank).
Conclusions
The degree of donor glomerular sclerosis has a major impact on graft function and survival and appears to be the best predictor of outcome of all other donor factors. The findings of this study indicate that a routine biopsy should be performed at the time of procurement as its result may be relevant to the subsequent allocation of a cadaveric kidney
Insurance Issues in Living Kidney Donation
Sarah Clarke, Jen A Lumsdaine, Stephen J Wigmore, Murat Akyol, John LR Forsythe.
Transplant Unit, Royal Infirmary of Edinburgh, Lauriston Place, Edinburgh, EH3 9YW
Objective: To investigate attitudes of the United Kingdom insurance industry to life and health insurance provision to living kidney donors.
Design: Questionnaire based surgery.
Setting: United Kingdom
Participants: 39 life and health insurance providers.
Main outcome measures: Identification of variance of insurance practice for living kidney donors compared with standard practices.
Results: Responses were received from insurers providing 79% of UK life insurance market. All but one insurer confirmed that they would pay the agreed life insurance sum if a customer should die as a consequence of live donation and all would accept new customers who had previously donated a kidney. The timing of acceptance of new customers after donation varied among both life and health insurance companies. Further variations were identified among health insurers regarding premiums and cover of the cost of donor investigations and operation.
Conclusion: Existing life insurance cover appears to be adequate for living kidney donors. There are variations in the timing of acceptance of new customers for life and health insurance after kidney donation. Standardisation and the use of objective criteria for the assessment and acceptance of new customers, who have previously donated a kidney, by insurers is desirable and would alleviate many of the concerns of individuals who have or are considering living kidney donation.
Peter Medawar in Glasgow, 1942
David Hamilton
Transplant Unit, Western Infirmary, Glasgow
A Journal of Anatomy paper in 1943 from Glasgow's Royal Infirmary by the local surgeon
Tom Gibson and the visiting scientist Peter Medawar is usually taken as the starting point of the modern understanding of tissue transplantation. Their work, though on a single human burns case, suggested that homograft/allograft rejection was a general phenomenon. They also demonstrated a 'second set' response in repeated human skin grafting, concluding that an immunological mechanism was involved.
Medawar's dominance later would suggest that Gibson had only a supporting role, but study of the evidence from the time shows instead that Gibson was the activist. Study of the data also reveals a more complex clinical situation, and some puzzles which can be explained by a chance full match of the recipient and the sib skin donor, and the likely low host reactivity of the badly-burned recipient. The two investigators may also have been lucky to find evidence of accelerated rejection of the second set of grafts, a finding others found difficult to confirm later. The absence of a cellular infiltrate also led Medawar to adhere for some time thereafter to a humoral explanation of graft rejection.
Malignant melanoma in renal transplantation
Junor BJR, Reid R, MacKie R. Dermatology, Pathology and Nephrology, Western Infirmary,
Glasgow
Over one year after a cadaver transplant a 56 year old female developed a breast lump which was thought to be an atypical breast tumour. Skin lesions and a mass in the transplanted kidney subsequently occurred. A biopsy of the transplant revealed malignant melanoma. Despite withdrawal of immunosuppression she deteriorated rapidly and died.
A few months later a 66 year old male transplant recipient also developed a mass in the transplanted kidney which on biopsy was also malignant melanoma. Both kidneys had come from the same donor, a 61 year old female who had died following an intracerebral haemorrhage. There was no history given of malignant melanoma at that time.
Subsequent investigation showed that she had had a malignant melanoma completely excised from her forearm 16 years before.
Immunosuppression was withdrawn and interferon-alpha given to induce a rejection process to attempt to destroy the melanoma cells as well as the transplant. Transplant nephrectomy was delayed for as long as possible. He is alive more than 2 years later and is being reconsidered for transplantation.
Revascularisation of cadaveric kidney transplant following renal artery occlusion secondary to angioplasty
Subramaniam M, Edwards R, Osman HY
Department of Surgery, Western Infirmary, Glasgow
Department of Radiology, Gartnavel General Hospital, Glasgow
Abstract:
Arterial thrombosis causing complete occlusion is a rare event in the natural history of a transplanted allograft; an incidence of 1.4% has been reported. It usually results from technical problems, hyper-acute rejection, severe atherosclerosis or injury to donor or recepient arteries for which the treatment of choice is transplant nephrectomy.
A significant renal artery stenosis was detected on duplex scanning eight month following a cadaveric renal transplant. Angiography and angioplasty were performed. This resulted in a complete occlusion of the external iliac artery and the transplant renal artery.
We report a scenario where the graft and lower limb were successfully salvaged.
The key factors were early resuscitation and aggressive surgical management.
Treatment and outcome of patients with primary focal segmental glomerulosclerosis and nephrotic syndrome in five UK renal units.
1 CM. Stirling, 2 P. Mathieson, 3 J.M. Boulton-Jones, 4 J. Feehally, 5 D. Jayne and 6 D. Adu ,
1
Glasgow Western Infirmary,
2
Southmead Hospital, Bristol,
3
Glasgow Royal Infirmary,
Hospital ,
5
St Helier Hospital,
6
Queen Elizabeth Hospital, Birmingham.
4
Leicester General
Focal segmental glomerulosclerosis (FSGS) is the least studied of the causes of idiopathic nephrotic syndrome and there are no clear guidelines for treatment. We reviewed data from 5 UK renal units in order to establish whether patients with FSGS were treated uniformly and to examine the effect of treatment on proteinuria and survival. One hundred and thirty nine patients with primary FSGS and nephrotic syndrome were included. Seventy nine patients (57%) were treated with prednisolone. The median duration of treatment with prednisolone varied from 6 months to 24 months. Twenty six patients were given cyclophosphamide, 26 cyclosporin and 20 azathioprine in addition to steroids. The overall remission rate was 65% but varied from 42-80% in the 5 units.
Twenty three percent of patients in both the treated and untreated groups developed ESRF but a greater number of patients died in the untreated group (15% v 1%). There was therefore a trend to improved overall survival in the treated group. The majority of patients who developed ESRF were those who had failed to respond to treatment. Only 3 patients (6%) who went into total or partial remission developed ESRF in comparison to 15 patients (58%) in the group who failed to respond (Graph 1). The unit which gave the most steroids had the best results. There was little difference in the treatment effects of additional cytotoxics.
Treatment with corticosteroids improves outcomes in patients with FSGS and nephrotic range proteinuria but further clarification of optimal treatment requires a multi-centre randomised control trial (RCT).
Graph 1: Survival in treated (remission), treated (no remission) and untreated groups
Treated, in remission
Untreated
Treated, no remission
Log rank p<0.0001
The epidemiology of Acute renal failure in Scotland (ARFS); - the story continues.
J Baharani 1 , H Martin 1 , L Lawson 1 , W Metcalfe 1 , W Smith 2 , K Simpson 3 , A MacLeod 1 , and I Khan 1
1 Department of Medicine and Therapeutics University of Aberdeen, 2 Department of Public Health
University of Aberdeen, 3 Scottish Renal Registry Glasgow
There are few population based epidemiological data on ARF requiring RRT. The Acute Renal Failure Scotland study
(ARFS) is registering adult patients all over Scotland with ARF, acute on chronic renal failure or CRF receiving their first
RRT over a 9- month period. The aim is to establish the incidence of ARF requiring RRT in a defined population base and to determine the factors affecting both the incidence of ARF treated by RRT and the outcome of such patients over a 90day period. All adult patients in Scotland receiving their first RRT are identified by regular phone calls and visits to all
Scottish hospitals offering this treatment. For the purpose of data collection we have broadly divided Scotland into 3 regions as shown in the figure 1.Over a 24 week period we have collected data on 563 patients who started RRT for either acute renal failure or acute on chronic renal failure. We also have data on all patients who started RRT for CRF.
The breakdown of the data is shown in table below.
Fig 1
Number of ARF
Number of ACRF
(acute on chronic)
Total
Number of Hospitals
Population base
Incidence of acute and acute on chronic RRT p.m.p/year
NORTH
139
22
161
3
1 200 500
268.2
SOUTH-EAST
109
46
155
6
1 373 900
225.6
WEST
177
70
247
11
2 548 100
193.9
Of the 563 patients, 61% are male and the average age is
62.1years.
The majority of patients receiving RRT for ARF are in the 66-80 age group and over 50% of RRT for ARF occurs outside the renal unit.
The overall incidence of ARF requiring RRT in Scotland is over 200 p.m.p/year
Our ongoing study of a known population shows that the incidence of ARF requiring RRT is higher than that reported by previous retrospective UK community based studies. The study is currently in its final phase of data collection.
Intensive Medical Management in Type 2 Diabetes and Nephropathy: Renal
Consequences
Nicola Joss, Christine Brown, Caroline Ferguson, Michael Boulton-Jones
Renal Unit, Glasgow Royal Infirmary, Glasgow
Ninety patients with type 2 diabetes and diabetic nephropathy were enrolled in a randomised controlled study comparing the intensity of medical treatment on the rate of progression of renal failure. The 47 patients randomly allocated to the intensive group (IG) were seen as often as necessary to meet various targets. These targets were identical for the
43 patients in the control group (CG) who were seen at their normal clinic. The primary endpoint was the rate of progression in the second year. Data from 3 monthly clinic visits were analysed. The creatinine clearance (ECC) was determined using the Cockcroft and
Gault formula and the rate of decline in renal function was calculated from linear regression of the slope of the plot of ECC versus time.
At baseline the 2 groups were well matched, the mean age was 63 years, BP 165/87 mmHg,
HbA
1c
7.9%, cholesterol 5.5 mmol/l, ECC 55 ml/min and median albumin:creatinine ratio
(ACR) 79 mg/mmol. Significant improvements were seen in the IG between baseline and 2 years with absolute reductions in SBP of 22 mmHg (p<0.01), DBP 15 mmHg (p<0.01), sodium intake 27 mmol/day (p=0.02) and cholesterol 1.3 mmol/l (p<0.01). In the CG significant improvements in DBP and cholesterol were seen with absolute reductions of 5 mmHg (p <0.01) and 0.9 mmol/l (p<0.01) respectively. At two years the IG had significantly lower SBP (p<0.01), DBP (p<0.01) and cholesterol (p=0.04). There was no difference in glycaemic control, protein intake or ACR either between the two groups at the end of the study or within the individual groups between baseline and 24 months. The median number of visits in the IG was 19 and 8 in the CG.
The rate of progression in both groups was not significantly different in year 1 (IG 0.44 ml/min/month vs CG 0.5 ml/min/month. A reduction was seen in the rate of progression of renal failure in the IG in year 2. (IG 0.14 ml/min/month vs CG 0.53 ml/min/month, p=0.04). The benefit of this can be calculated in terms of delay in starting dialysis. The mean ECC at baseline was 55 ml/min, assuming the rates of progression achieved in the second year persisted, the average time to starting dialysis would be 27 years in the intensive group and 7 years in the control group. The savings from this may offset the extra costs of clinics.
An analysis of co-morbidity and survival in patients registered for the renal transplant waiting list
R.F. Jeffrey, H. Akbani, A.J. Scally, Department of Renal Medicine, St. Lukes Hospital,
Bradford and School of Health Studies, University of Bradford.
The decision to list a patient for transplantation must reconcile the desire to provide best care to the individual with the responsibility to utilise a scarce resource appropriately.
This involves a careful assessment of co-morbid risk in patients being considered for the national transplant waiting list. Since the opening of the Bradford renal unit in 1994, 213 adult patients have been accepted for renal replacement therapy up until 31 December
2000. We have retrospectively assessed the decision to list or not with regard to age and co-morbidity, and evaluated patient survival by Kaplan-Meier analysis (data censored at
31 December 2001).
With regard to listing the following were excluded prior to further analysis: 18 patients with either myeloma or solid malignant tumours within 5 years of diagnosis; 3 through self choice; 4 with significant sociopathy and 3 who died during work-up. The remaining
185 patients were analysed in greater detail. There were 109 males and 63 of Indo-Asian ethnic background. The following co-morbid factors were recorded - diabetes mellitus (46 patients), ischaemic heart disease (IHD) (42), peripheral vascular disease (PVD) (24), cerebrovascular disease (CVD) (19), obesity (BMI > 30) (21). During this period 102 patients (55%) were listed for transplantation.
According to the co-morbidity stratification of Khan et al. (Lancet, 341; 415:1993), 86 patients were low risk of whom 87% were listed, 50 were medium risk with 46% listed, and 48 were high risk with only 8% listed. A logistic regression model was applied to determine which factors were of importance in listing decisions. Ethnic group and gender did not predict listing. The most influential factors in the model against listing were age
>60 and >70 years, diabetes, liver disease, CVD and PVD with IHD being less important after including the other factors.
There was a highly significant difference in survival according to listing decision
(p<0.0001 by log rank test). Survival at 1 and 5 years was 0.98 (CI 0.92-1.00) and
0.81(0.69-0.89) in those listed and 0.71(0.62-0.79) and 0.22(0/11-0.34) in those never listed. Fifty patients received a graft during the observation period. Of those listed 17 have died, 3 having been transplanted. Only 3 others were active on the waiting list at the time of death. An important criterion for registration of patients is an expectation of survival for a number of years if transplanted. A listing strategy which takes account of co-morbidity has clearly identified a cohort with low medium term mortality. It is gratifying that so few patients died with functioning grafts.