journal_onpreeclampsia
advertisement

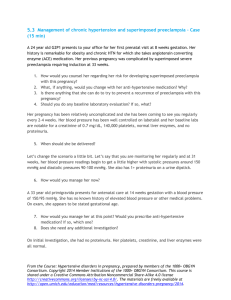
LaGuardia Community College City University of New York Department of Natural & Applied Science Practical Nursing Program Written Report: “Preelampsia: Exposing Future Cardiovascular Risk in Mothers and Their Children” By Anaise E. Ikama Course: SCL 115 – Maternal Child Health Nursing Professor: Maureen Griffith It has long been suggested that mothers often are the reason why children carry certain diseases. Though, it may be the case for some maladies, early assessment and identification of these illnesses from the mother during pregnancy can provide enhanced prevention opportunities to the child. Recently, researchers have been focusing their attentions on the fetal origins of cardiovascular disease and preeclampsia. Preeclampsia, according to the Journal of Obstetric, Gynecologic & Neonatal Nursing is defined as “a pregnancy – specific syndrome characterized by new-onset hypertension (systolic blood pressure greater than 140 mm Hg or diastolic blood pressure greater than 90 mm Hg) during the second half of pregnancy, coupled with proteinuria greater than 300 mg per 24-hour sample (Anderson. JOGNN, volume 36, pp 3). In the Journal of Obstetric, Gynecologic & Neonatal Nursing (JOGNN), the article “Preeclampsia: Exposing Future Cardiovascular Risk in Mothers and Their Children”, the editor Cindy M. Anderson examines the influence of fetal development and maternal preeclampsia as they correlate to the development of future cardiovascular risk in mothers and their children. With the placenta ruling both the mother and the baby, it has now been associated with the development of preeclampsia; in which maternal spiral arteries that provide the blood supply to the placenta is inadequate, limiting blood flow to the placenta as well as to the fetal causing vasoconstriction of the arteries and increased pressure of the circulating blood. The characteristic clinical manifestations of preeclampsia, which include headache, reduced glomerular filtration, blurred vision/scotoma, and fetal growth restriction also contributes to arterial vasoconstriction that reduces perfusion to multiple organ system. Therefore, if the fetal metabolic function adapt to the reduced placental 1 flow, it may lead to adult-onset diseases such as hypertension and coronary artery disease. Not only are arterial vasoconstriction related to preeclampsia, but also are nonpregnant women with impaired endothelium-independent vasodilation with a history of preeclampsia compared to non-pregnant women who did not experience pregnancy complicated by preeclampsia; providing a plausible explanation for increased risk for the development of hypertension. More than 75, 000 women, out of a million, in the study who had no CV disease prior to their first pregnancy developed a placental abruption during their pregnancy. Researchers have concluded that the first trimester was the period most likely to result in increased CV risk when fetals were affected by maternal malnutrition. As Anderson affirms on page 5, “Fetal nutrition, or the supply of metabolic substrates delivered for growth and development, contributes…intrauterine growth restriction and low birth weigh, childhood obesity, hypertension, and diabetes.” Children born from mothers with preeclampsia are prone to a higher risk for developing hypertension and other adult diseases later in life. Statistically speaking, the risk for preeclampsia in primigravida was 37% among sisters and 27% among daughters of women with eclampsia. Interestingly, exposure to preeclampsia in utero has increased the risk for preclampsia in both sons and daughters. And among these kids who have been exposed to preeclampsia in utero, daughters were twice likely to develop preeclampsia themselves. Childhood blood pressure provide an opportunity to identify future hypertensions, therefore, to prevent risk for cardiovascular in mothers and their children, the Seventh Report of the Joint National Committee on Prevention, Detection and Evaluation and 2 Treatment of High Blood Pressure (JNC 7) specified that for an increase of 20 mm Hg increment in systolic and 10 mm Hg increment in diastolic blood pressure, starting at 115/75, there is a chance of developing CV. Though, it may affect a small population of pediatric, we should think about the long-term consequences of this cardiovascular disease that will burden at these children as they become older. Choosing this article was like exposing oneself to a place full of opportunities. Most of my life I have seen pregnant women suffering with heart problem and others handed having heart problem during postpartum. I always wonder if the fundus was the causative agent of cardiovascular disease during pregnancy. And writing about this article has helped me differentiate between cardiovascular disease before and during pregnancy. All in all, exposure of CV risk due to preeclampsia may cause hypertension secondary to the stress of additional demands of pregnancy. As future nurses, we have these unique opportunities to act both as health care providers and teachers; therefore, we should utilize our talents to educate pregnant women or women that are planning to become pregnant about preeclampsia and its exposure to cardiovascular risk. A plan of care for optimal cardiovascular health must be established, to reduce the danger of preeclampsia in the developing fetus. Let’s not forget that “the opportunities to enhance the health of future generations begin with care of pregnant women to address the fetal origins of disease” (Anderson. JOGNN, Volume 36, pp 7). 3 WORKED CITED Cindy M. Anderson. “Preeclampsia: Exposing Future Cardiovascular Risk in Mothers and Their Children”. (2007). Journal of Obstetric, Gynecologic & Neonatal Nursing, Volume 36 pp3-7. Retrieved September 11, 2007, from http://www.blackwell-synergy.com/toc/jogn/36/ 4