Please insert here the title of your abstract
advertisement

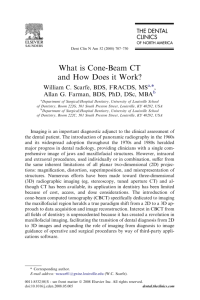
Extraction of the respiratory signal from sequential thorax Cone-Beam X-ray images Lambert Zijp, Jan-Jakob Sonke, Marcel van Herk The Netherlands Cancer Institute / Antoni van Leeuwenhoek Hospital, Amsterdam, The Netherlands Abstract Cone-Beam CT (CBCT) scans of the thorax and upper abdomen contain considerable artifacts caused by respiratory motion. These artifacts can be prevented in CBCT if only those X-ray images that are obtained during the same breathing phase are used for subsequent reconstruction. In this paper, a method is presented to determine the breathing signal from the X-ray images themselves, thus obliterating the use of respiration sensors and the need to synchronize breathing signal measurements with image acquisition. The method is fast, robust and fully automatic. The principal idea in the method is to enhance diaphragm like features in the individual X-ray images, project these features on the cranio-caudal axis, combine all successive 1D projections to a 2D image, and to extract from this image features that change position along the cranio-caudal axis. Keywords Cone-Beam CT, 4D radiotherapy, X-ray, projections, thorax, diaphragm, reconstruction artifacts, breathing cycle Introduction A prerequisite for high quality CT reconstructions is that enough angular projections are made and that the scanned object is stationary [1,2,3]. In medical imaging the latter condition is not always met. Especially CT scans of the thorax and upper abdomen contain huge artifacts due to breathing motion within the patient. In spiral CT scanners, an X-ray source and a 1D detector rotate with high speed around the patient, and the patient moves slowly through the scanner. This gives rise to a sequence of sharp 2D axial reconstructions. In areas where breathing motion is large, the 3D combination of these images contains spatial distortions (Fig 1 left). In Cone-Beam CT (CBCT) scanners, an X-ray source and a 2D detector rotate slowly around a stationary patient and typically collect 300-1000 images [4]. The detector produces sharp 2D conical projections, but the 3D reconstruction will be blurred in areas with large breathing motion (Fig 1 right). acquisition result in 3D reconstructions of diagnostic quality, but impair the patients comfort, may increase the scanning time, and may be too a-typical of the patients behavior for satisfactory use in radiotherapy. Another strategy is to let the patient breathe freely, and select for 3D reconstruction only those images that were made in the same phase of the breathing cycle. Following this scheme, and having acquired a sufficient amount of images, permits a 4D reconstruction [6,7,8]. The breathing signal can be determined by measurement of temperature differences between inhaled and exhaled air near the patients nose, by measurement of changes in the circumference of the thorax using stretch sensors, or using reflective markers on the patients chest. These types of measurements need to be synchronized with the exact time at which individual slices were acquired in the spiral CT, or at which X-ray images were taken in a CBCT scanner. This paper presents a method to extract the breathing signal from the individual X-ray images in a CBCT acquisition sequence. A thus obtained breathing signal is synchronized by definition, and eliminates the need for additional equipment. Material and methods Figure 1: Breathing artifacts in the lower lung: distortion in conventional CT (left) and blurring in CBCT (right). For both CT scanning techniques, methods have been proposed to prevent these breathing artifacts from occurring. Breath holding during the whole scanning period or operator controlled breathing [5] combined with interrupted image The CBCT scanner used was an Elekta Synergy Research Platform, consisting of a conventional 120kV X-ray source and an a-Si detector, both mounted on the gantry of an Elekta SL20i linac. The source-detector distance was 153.6 cm; the detector has a field of view of 25.6cm by 25.6 cm at the isocenter plane; radiation exposure is about 50μGy per image, given in an X-ray pulse of 20msec. During a 360 degree rotation around the patient (which takes 2-4 minutes), 330 to 660 images with a 512x512 resolution, were acquired. Algorithm All X-ray transmission images underwent a few processing steps in order to highlight the diaphragm. This processing can be done during acquisition of subsequent images. The diaphragm is the most prominent anatomical structure exhibiting breathing motion, and its position is assumed to be a good measure for the breathing phase. First, the logarithm of the images was taken (Fig 2 left); the pixel values then become proportional to the radiological thickness. The position of the diaphragm is characterized by a steep cranio-caudal (CC) transition from light to dark. Applying a CC derivative filter emphasizes this feature (Fig 2 right). Figure 2: The logarithm of a CBCT X-ray image (left), and its CC derivative (right). The prominent vertical bar in the middle of the logarithmic image, is one of the two carbon fiber reinforced table-support arms entering the field of view. Vertical features like these disappear when using a CC derivative filter. A threshold was first applied to the logarithmic image to discern patient from air, and next to its CC derivative to isolate diaphragm-like transitions. The results are combined to mask interesting regions in a gradient filtered image (Fig 3 left). The enhanced X-ray images are projected on the CC axis, and all the 1D projections are then combined and depicted as a 2D image: the ‘Amsterdam Shroud’ (Fig 4). In this image, the columns are the 1D CC projections of successive enhanced images. Note that regions of high intensity are relatively stationary in time, except for the diaphragm region, which clearly manifests itself as a more or less periodic signal in the caudal part of the shroud. Figure 4: The ‘Amsterdam Shroud’. Each column corresponds to a single projection image. In order to automatically detect this region, the temporal derivative (i.e. horizontal derivative) of the shroud is calculated. This operation enhances features that change in time, and lets stationary features disappear. The absolute value of the temporal derivative (Fig 5) is then again projected on the CC axis, resulting in a 1D signal exhibiting a very prominent peak indicating the region of the diaphragm. Figure 3: The enhanced X-ray image (left) and its projection on CC axis (right). In the resulting enhanced X-ray image, the presence of many other features like upper arms, patient to air transitions, and ribs, makes isolation of the diaphragm a formidable task. The method presented here does not try to isolate the diaphragm, but uses the fact that the diaphragm is the only feature that moves considerably! Figure 5: The absolute of the temporal derivative of the ‘Amsterdam Shroud.’. This region then, is cut out of the ‘Amsterdam Shroud’ and subjected to the final processing step. Each is column aligned to the next column, in such a way that the root mean square of all pixel value differences is minimized. The number of pixels that one column had to be shifted cranially or caudally for optimal fit is the respiration signal. In figure 6 the number of pixel shifts needed for each optimal pair-wise alignment are shown cumulatively. After removal of the low frequency components using a high-pass filter, the resulting signal is ready for 4D reconstruction purposes. Figure 6: The extracted breathing signal Figure 6: A sagittal (left) and a coronal (right) slice of a scan. The upper two are slices through one of the phase bins of a 4D CBCT reconstruction. The lower two are slices through a conventional 3D CBCT reconstruction. Results and discussion Conclusion Processing of all X-ray images can be done during image acquisition. Processing of the ‘Amsterdam Shroud’ takes a few seconds. The method has been tested on all available CBCT scans made in our institute, where the diaphragm was inside the field of view: one mamma patient, three lung patients, two upper abdomen patients, and one rabbit (kindly provided by the PMH in Toronto); 24 scans in total. The values of the few thresholds used for the first CBCT scan, did not need any alteration in order to work for subsequent scans. These ‘one size fits all’ parameters indicate robustness of the method. In all cases, a clear periodic signal was extracted. The signals were visually verified in two ways. Firstly by inspection of created movies, where the frames consisted of successive raw X-ray images in which vertical bars reflecting the extracted signal were inserted. These movies showed good correspondence between the moving bar and the position of the diaphragm. Secondly, the 4D reconstructions using phase bins of the extracted signals were inspected. Two 2D examples of a 4D reconstruction are shown in figure 7. The sharpness of the upper two slices indicate that the projections used to make the reconstruction belong more or less to the same breathing phase. Comparison of the extracted breathing cycle with thermometer measurements was not done, because any possible discrepancies between the two may very well be attributed to the thermometer being less fit for the purpose. A fast, robust and fully automatic method has been developed for determining the breathing phase of successive CBCT X-ray images of the thorax. The method has been successfully applied for respiration correlated CBCT reconstruction. References [1] J. Radon, Űber die bestimmung von funktionen durch ihre integralwerte längs gewisser mannigfaltigkeiten, Berichte Sächsische Akademie der Wissenschaften, 69:262-267 (1917). [2] L.A. Feldkamp, L.C. Davis, and J.W. Kress, Practical conebeam algorithm, J. Opt. Soc. Am. A 1, 612–619 (1984). [3] B.D. Smith, Image reconstruction from cone-beam projections: necessary and sufficient conditions and reconstruction methods, IEEE Trans. Med. Imag, MI-4:1428 (1985). [4] D.A. Jaffray, J.H. Siewerdsen, J.W. Wong, and A.A. Martinez, Flat-Panel Cone-Beam Computed Tomography for Image-Guided Radiation Therapy, Int. J. Radiat. Oncol. Biol. Phys. 53, 1337–1349 (2002). [5] L.W. Wong, M.B. Sharpe, D.A. Jaffray, V.R. Kini, J.M. Robertson, J.S. Stromberg, and A.A. Martinez, The use of active breathing control (ABC) to reduce margin for breathing motion, Int. J. Radiat. Oncol. Biol. Phys. 44, 911919 (1999). [6] S.S. Vedam, P.J. Keall, V.R. Kini, H.Mostafavi, H.P. Shukla, and R.Mohan, Acquiring a four-dimensional computed tomography dataset using an external respiratory signal, Phys. Med. Biol. 486, 45–62 (2003). [7] E.C. Ford, G.S. Mageras, E. Yorke, and C.C. Ling, Respiration-correlated spiral CT: A method of measuring respiratory-induced anatomic motion for radiation treatment planning, Med. Phys. 30, 88–97 (2003). [8] J. Sonke, P. Remeijer and M. van Herk, RespirationCorrelated Cone-Beam CT: Obtaining a Four-Dimensional Data Set (WIP), Med. Phys. 30, 1415 (2003).