Hospital Billing Tips
Provider Reference Supplement
HP Enterprise Services, Arkansas Title XIX
Document Date: 5/12/2010
HP Enterprise Services
Arkansas Title XIX Account
500 President Clinton Avenue, Suite 400
Little Rock, Arkansas 72201
(501) 374-6608
HP Enterprise Services and the HP Enterprise Services logo are registered trademarks of HP Enterprise
Services.
All other logos, trademarks or service marks used herein
are the property of their respective owners.
HP Enterprise Services is an equal opportunity employer and values the diversity of its people.
© 2010 HP Enterprise Services.
All rights reserved.
Contents
Contents.......................................................................................................................... 3
Introduction ..................................................................................................................... 5
Eligibility .......................................................................................................................... 6
Restricted Aid Categories ......................................................................................... 6
All Arkansas Medicaid Aid Categories ...................................................................... 9
Inpatient Hospital .......................................................................................................... 12
Exclusions .................................................................................................................. 13
Inpatient Hospital Services Benefit Limit .................................................................... 13
MUMP Applicability (Medicaid Utilization Management Program).................................. 14
MUMP Exemptions .................................................................................................... 14
MUMP Certification Request Procedure ..................................................................... 14
Arkansas Foundation for Medical Care Contact Information....................................... 15
Outpatient Hospital Services ......................................................................................... 16
Coverage ................................................................................................................... 16
Emergency Services .................................................................................................. 16
Benefit Limit for Emergency Services ..................................................................... 17
Non-Emergency Services .......................................................................................... 17
Outpatient Assessment in the Emergency Department .............................................. 17
Benefit Limit for Outpatient Assessment in the Emergency Department ..................... 18
Emergency, Non-Emergency and Related Charges ................................................... 18
Non-Emergency Charges ........................................................................................... 19
Laboratory, Radiology and Machine Test Services .................................................... 19
Benefit Limit in Outpatient Laboratory, Radiology and Machine Test Procedures ....... 20
Benefit Limits for Fetal Non-Stress Test and Fetal Ultrasound ................................... 20
Observation Bed Status ............................................................................................. 21
Observation Bed Policy Illustration ............................................................................. 21
Observation Bed Billing Information ........................................................................... 21
Benefit Limit for Non-Emergency Services ................................................................. 22
Billing for UB04 ............................................................................................................. 24
Most Common Inpatient Types of Bills: ...................................................................... 24
Type of Bill Code Structure – Three Digit Number ...................................................... 24
First Digit – Indicates Type of Facility ...................................................................... 24
Second Digit – Indicates Bill Classification .............................................................. 24
Third Digit – Indicates Frequency ........................................................................... 25
Admit Source Codes ............................................................................................... 25
Admit Source Codes (Newborn) ............................................................................. 26
Patient Status Codes .............................................................................................. 26
Condition Codes ........................................................................................................ 27
Condition Code crosswalk ...................................................................................... 27
Billing clarification: Inpatient claim type S 10/5/07 ...................................................... 27
Formula for determining total days for which to bill ..................................................... 27
eOB: 007-Total days not equal to the difference between the “From” and “To” Dates
............................................................................................................................... 27
Timely Filing ............................................................................................................... 28
Revenue Codes ......................................................................................................... 29
Hospital Billing Instructions – Paper Only ...................................................................... 42
Requesting Crossover Forms ........................................................................................ 48
Tips for Completing Crossover Forms ........................................................................... 49
3
Arkansas Medicaid Hospital Billing Tips
Outpatient Crossover .............................................................................................. 52
Inpatient Crossover ................................................................................................. 54
Common Billing Errors .................................................................................................. 55
Helpful Tips and Procedures ......................................................................................... 56
Levels of Emergency Claims ...................................................................................... 56
HP Enterprise Services Contact Information ................................................................. 57
4
Introduction
This Billing Tips document serves as a training supplement for Arkansas Medicaid
providers but does not supersede official program documentation, including the
following: Arkansas Medicaid Provider Reference manuals, Official Notices and
transmittal letters published by the Division of Medical Services and distributed by
HP Enterprise Services.
This document focuses on Arkansas Medicaid eligibility, common policy questions
and billing issues. This information is incorporated into the following quick reference
sections for your convenience:
Consolidated list of restricted aid categories
Hospital Inpatient
Hospital Outpatient, Emergent and nonemergency services
Paper claims submission instructions
Contacts
5
Arkansas Medicaid Hospital Billing Tips
Eligibility
Beneficiary eligibility for the Arkansas Medicaid program is determined at the
Department of Human Services (DHS) county office. A beneficiary’s eligibility may
begin and end on any day of any month. Because program eligibility is date specific,
providers are required to check each beneficiary’s eligibility on the date of service
and are encouraged to do so using one of the following tools:
PES
Arkansas Medicaid Direct Data Entry (DDE) website
Both tools verify eligibility electronically for a specific date or range of dates,
including retroactive eligibility for a year. For more information on eligibility, refer to
Section I of the Arkansas Medicaid provider manual.
Restricted Aid Categories
Many providers ask a question that is closely related to eligibility: “Is there a list of aid
categories that require a primary care physician?” The answer is no. Arkansas
Medicaid’s primary care case management program, ConnectCare, requires
Medicaid beneficiaries and waiver participants to enroll with a primary care physician
(PCP) unless specifically exempt from that requirement.
See these sections of your Arkansas Medicaid provider manual for more information
related to eligibility:
Section 171.000, which lists the groups of individuals who may not enroll with a
PCP
Section 176.000, which lists Medicaid covered services that do not require PCP
referral
On the following pages are a consolidated list of aid categories with restrictions and
a complete list of aid categories taken from Section 124.000 of your Arkansas
Medicaid provider manual.
6
The table below lists and briefly describes restricted aid categories. Post it at your
workstation to use as a convenient quick reference:
Aid Category
Restriction
01 ARKids First-B
Beneficiaries may have co-payment requirements.
(PCP Required)
Beneficiaries may be ineligible for certain services
(see the ARKids First-B provider manual for
exclusions.)
03 CMS (Children’s Medical
Services)
All services must be prior authorized by the CMS
office.
Non-Medicaid
(No PCP Required)
04 DDS (Developmental
Disability Services)
DDS non-Medicaid provider ID numbers end with
‘86’.
Non-Medicaid
DDS non-Medicaid beneficiary ID numbers begin
with ‘8888’.
(NO PCP Required)
Only DDS non-Medicaid providers may bill for DDS
non-Medicaid beneficiaries.
DDS beneficiaries may be dually eligible and
receive additional services in another category.
*6 Medically Needy
Exceptional
Beneficiaries are eligible for a full range of benefits
except nursing facility and personal care.
(PCP Required)
*7 Spend Down
(No PCP Required)
(PCP required for Breast
Care, 07)
08 Tuberculosis
(NO PCP Required)
Beneficiaries must pay toward medical expenses
when income and resources exceed the Medicaid
financial guidelines.
Note: Aid category 07 BCC has full benefits.
Beneficiary coverage includes drugs, physician
services, outpatient services, rural health clinic
encounters.
Federally Qualified Health Center (FQHC) and clinic
visits for TB-related services only.
7
Arkansas Medicaid Hospital Billing Tips
Aid Category
Restriction
*8 QMB (Qualified Medicare
Beneficiary)
Medicaid pays Medicare premiums, coinsurance
and deductible.
(No PCP Required)
If the service provided is not a Medicare covered
service, Medicaid will not pay for the service under
the QMB policy.
Note: Aid category 18 S has full benefits.
61 PW-PL (Pregnant Woman
Infants and Children Poverty
level)
This category contains both pregnant women and
children. Providers must use the last three-(3) digits
of the Medicaid ID number to determine benefits.
(No PCP Required For
Pregnant Woman)
When the last three (3) digits are in the 100 series
(i.e., 101, 102, etc.), the beneficiary is eligible as an
adult and is eligible for pregnancy-related services
only.
(PCP Required for the Infants
and children)
When the last three (3) digits are in the 200 series
(i.e., 201, 202, etc.), the beneficiary is eligible as a
child and receives a full range of Medicaid services.
Note: Plan description “PW unborn ch-noster/FP
cov” indicates there is no sterilization or
family planning benefits for the expectant
mother.
62 PW-PE (Pregnant Woman
Presumptive Eligibility)
A temporary aid category that pays for ambulatory,
prenatal services only.
(No PCP Required)
69 Women’s Health Wavier
(No PCP Required)
Medicaid pays for family planning preventative
services only, such as birth control or counseling.
A claim for a beneficiary in this category must
contain both a family planning diagnosis code and a
family planning procedure code.
58, 78, 88 SLIMB (Specified
Low Income Medicare
Beneficiary)(SMB)
Medicaid pays only their Medicare premium.
(No PCP Required)
8
All Arkansas Medicaid Aid Categories
The following is the full list of beneficiary aid categories. Some categories may
provide a full range of benefits, limited benefits or may be a category that requires
cost sharing by a beneficiary. The following codes describe each level of coverage.
FR - Full range
LB - Limited benefits
AC - Additional cost sharing
MNLB - Medically needy limited benefits
Category
Description
Code
01 ARKIDS B
ARKids First Demonstration
LB, AC
07 BCC
Breast and Cervical Cancer Prevention and
Treatment
FR
08 TB-Limited
Tuberculosis – Limited Benefits
LB
10 N WD NewCo
Working Disabled – New Cost Sharing (N)
FR, AC
10 R WD RegCo
Working Disabled – Regular Medicaid Cost
Sharing I
FR, AC
11 AABD
AABD
FR
13 SSI
SSI
FR
14 SSI
SSI
FR
16 AA-EC
AA-EC
MNLB
17 AA-SD
Aid to the Aged Medically Needy Spend
Down
MNLB
18 QMB-AA
Aid to the Aged-Qualified Medicare
Beneficiary (QMB)
LB
18 S AR Seniors
ARSeniors
FR
20 AFDC-GRANT
Transitional Employment Assistance (TEA,
formerly AFDC) Medicaid
FR
25 TM
Transitional Medicaid
FR
26 AFDC-EC
AFDC Medically Needy Exceptional
Category
MNLB
27 AFDC-SD
AFDC Medically Needy Spend Down
MNLB
31 AAAB
Aid to the Blind
FR
33 SSI
SSI Blind Individual
FR
34 SSI
SSI Blind Spouse
FR
35 SSI
SSI Blind Child
FR
9
Arkansas Medicaid Hospital Billing Tips
Category
Description
Code
36 AB-EC
Aid to the Blind-Medically Needy Exceptional
Category
MNLB
37 AB-SD
Aid to the Blind-Medically Needy Spend
Down
MNLB
38 QMB-AB
Aid to the Blind-Qualified Medicare
Beneficiary (QMB)
LB
41 AABD
Aid to the Disabled
FR
43 SSI
SSI Disabled Individual
FR
44 SSI
SSI Disabled Spouse
FR
45 SSI
SSI Disabled Child
FR
46 AD-EC
Aid to the Disabled-Medically Needy
Exceptional Category
MNLB
47 AD-SD
Aid to the Disabled-Medically Needy Spend
Down
MNLB
48 QMB- AD
Aid to the Disabled-Qualified Medicare
Beneficiary (QMB)
LB
49 TEFRA
TEFRA Waiver for Disabled Child
AC
51 U-18
Under Age 18 No Grant
FR
52 ARKIDS A
Newborn
FR
56 U-18 EC
Under Age 18 Medically Needy Exceptional
Category
MNLB
57 U-18 SD
Under Age 18 Medically Needy Spend Down
MNLB
58 QI-1
Qualifying Individual-1 (Medicaid pays only
the Medicare premium.
LB
61 PW-PL
Women’s Health Waiver - Pregnant Women,
Infants & Children Poverty Level (SOBRA).
A 100 series suffix (the last 3 digits of the ID
number) is a pregnant woman; a 200 series
suffix is an ARKids-First-A child.
LB (for
the
pregnant
woman
only)
FR (for
SOBRA
children)
61 PW “Unborn
Child”
Pregnant Women PW Unborn CH-no Ster
cov – Does not cover sterilization or any
other family planning services.
LB (for
the
pregnant
woman
only)
62 PW-PE
Pregnant Women Presumptive Eligibility
LB
63 ARKIDS A
SOBRA Newborn
FR
65 PW-NG
Pregnant Women No Grant
FR
10
Category
Description
Code
66 PW-EC
Pregnant Women Medically Needy
Exceptional Category
MNLB
67 PW-SD
Pregnant Women Medically Needy Spend
Down
MNLB
69 FAM PLAN
Women’s Health Waiver (Family Planning)
LB
76 UP-EC
Unemployed Parent Medically Needy
Exceptional Category
MNLB
77 UP-SD
Unemployed Parent Medically Needy Spend
Down
MNLB
80 RRP-GR
Refugee Resettlement Grant
FR
81 RRP-NG
Refugee Resettlement No Grant
FR
86 RRP-EC
Refugee Resettlement Medically Needy
Exceptional Category
MNLB
87 RRP-SD
Refugee Resettlement Medically Needy
Spend Down
MNLB
88 SLI-QMB
Specified Low Income Qualified Medicare
Beneficiary (SMB) (Medicaid pays only the
Medicare premium.)
LB
91 FC
Foster Care
FR
92 IVE-FC
IV-E Foster Care
FR
96 FC-EC
Foster Care Medically Needy Exceptional
Category
MNLB
97 FC-SD
Foster Care Medically Needy Spend Down
MNLB
11
Arkansas Medicaid Hospital Billing Tips
Inpatient Hospital
Inpatient hospital services are defined in the Arkansas Medical Assistance Program
as those items and services ordinarily furnished by the hospital for care and
treatment of inpatients and are provided under the direction of a licensed practitioner
(physician or dentist with staff affiliation) of a facility maintained primarily for
treatment and care of injured, disabled or sick persons. Such inpatient services must
be medically justified, documented, certified and re-certified by the Quality
Improvement Organization (QIO) and are payable by Medicaid if provided on a
Medicaid-covered day.
A Medicaid-covered day is defined as a day for which the beneficiary is Medicaid
eligible, the patient’s inpatient benefit has not been exhausted, the patient’s inpatient
stay is medically necessary, the day is not part of a hospital stay for a non-payable
procedure or non-authorized procedure and the claim is filed on time. See Section III
of your provider manual for reference to “Timely Filing.”)
The following services are covered inpatient hospital services if medically necessary
for treatment of the patient and if the date of service is a Medicaid-covered day:
A. Accommodation - The type of room provided for the patient while receiving
inpatient hospital services. The Medicaid Program will cover the semi-private
room or ward accommodations and intensive care. A private room will only be
covered when such accommodations are medically necessary, as certified by the
patient’s attending physician. Private rooms are considered medically necessary
only when the patient’s condition requires him or her to be isolated to protect his
or her health or welfare or to protect the health of others.
B. Operating Room - Operating room charges for services and supplies associated
with surgical procedures are covered inpatient hospital services.
C. Anesthesia - Anesthesia charges for services and/or supplies furnished by the
hospital are covered inpatient hospital services.
D. Blood Administration - Blood, blood components and blood administration
charges are covered when not available to the beneficiary from other sources.
Hospitals are encouraged to replace blood that is used by a Medicaid beneficiary
through his or her friends and relatives or through the Red Cross whenever
possible.
E. Pharmacy - Drugs and biologicals furnished by the hospital for the care and
treatment of patients are covered inpatient hospital services. Take-home drugs
are non-covered inpatient hospital services under the Arkansas Medicaid
Program.
F. Radiology and Laboratory - The coverage of inpatient hospital services includes
the non-physician services related to machine tests, laboratory and radiology
procedures provided to inpatients. The hospital where the patient is hospitalized
will be responsible for providing or securing these services. The party who
furnishes these non-physician services is permitted to bill only the hospital.
If a patient is transferred to another hospital to receive services on an outpatient
basis, the cost of the transfer is included in the hospital reimbursement amount.
The ambulance company may not bill Medicaid or the beneficiary for the service.
G. Medical, Surgical and Central Supplies - Necessary medical and surgical
supplies and equipment that are furnished by the hospital for the care and
12
treatment of patients are covered inpatient hospital services. Supplies and
equipment for use outside the hospital are not covered by Medicaid.
H. Physical and Inhalation Therapy - Physical and inhalation therapy and other
necessary services, as well as supply charges for these services that are
furnished by the hospital, are covered inpatient hospital services.
I.
Delivery Room - Delivery room charges for services and supplies associated with
obstetrical procedures are covered inpatient hospital services.
J. Other – Other non-covered services not specified above.
Exclusions
The following items are not covered as inpatient hospital services:
A. Beauty shop
B. Cot for visitors
C. Meals for visitors
D. Television
E. Telephone
F. Guest tray
G. Private duty nurse
H. Take-home drugs and supplies
I.
Services not reasonable or necessary for the treatment of an illness or injury
J. Private room (unless physician certifies that it is medically necessary or unless
no semi-private rooms are available)
K. Autopsies
Medicaid does not cover services that are cosmetic, experimental, not medically
necessary or that are not generally accepted by the medical profession. Medicaid
does not cover services that are not documented by diagnoses that certify medical
necessity. Arkansas Medicaid has identified some ICD-9-CM diagnosis codes that
do not certify medical necessity. See sections 272.460 and 272.470 of the Hospital
provider manual for diagnosis codes that are not covered by Arkansas Medicaid.
Inpatient Hospital Services Benefit Limit
A. There is no benefit limit for acute care/general and rehabilitative hospital inpatient
services for beneficiaries under age 21 in the Child Health Services (EPSDT)
Program. Inpatient services must be approved by the QIO as medically
necessary.
B. The benefit limit for acute care/general and rehabilitative hospital inpatient
services is 24 paid inpatient days per state fiscal year (July 1 through June 30)
for Medicaid beneficiaries aged 21 and older.
C. Extension of the 24-day inpatient benefit is unavailable.
D. Inpatient stays that are prior authorized for heart, liver and lung transplants are
not counted toward the 24-day inpatient benefit limit.
13
Arkansas Medicaid Hospital Billing Tips
MUMP Applicability (Medicaid Utilization Management
Program)
A. Medicaid covers up to 4 days of inpatient service with no certification
requirement, except in the case of a transfer, subject to retrospective review for
medical necessity.
B. If a patient is not discharged before or during the fifth day of hospitalization,
additional days are covered only if certified by Arkansas Foundation for Medical
Care (AFMC).
C. When a patient is transferred from one hospital to another, the stay must be
certified from the first day.
MUMP Exemptions
A. Medicaid beneficiaries under age 1 at the time of admission are exempt from
MUMP requirements for dates of service before their first birthday.
B. The MUMP does not apply to inpatient stays for bone marrow, liver, liver/bowel,
heart, lung, skin and pancreas/kidney transplant procedures.
C. When there is primary coverage by a third party resource and the provider seeks
secondary coverage by Medicaid, Medicaid covers the same number of inpatient
days as the primary resource whether the number of covered days is less than,
equal to or greater than four. Therefore, MUMP certification is not required in
this circumstance.
MUMP Certification Request Procedure
When a patient is transferred from another hospital or when a patient’s attending
physician determines the patient should not be discharged by the fifth day of
hospitalization, utilization review or case management personnel may contact AFMC
and request an extension of inpatient days. See section 212.530 of the Hospital
provider manual for more information.
A. The following information is required:
1. Patient name and address (including ZIP code)
2. Patient birth date
3. Patient Medicaid number
4. Admission date
5. Hospital name
6. Hospital provider identification number
7. Attending physician provider identification number
8. Principal diagnosis and other diagnoses influencing this stay
9. Surgical procedures performed or planned
10. The number of days being requested for continued inpatient care
11. All available medical information justifying or supporting the necessity of
continued stay in the hospital.
14
B. AFMC may be contacted between 8:30 a.m. and 5:00 p.m., Monday through
Friday, except state holidays. Calls are limited to 10 minutes to allow equal
access to all providers.
C. Calls for extension of days may be made at any time during the inpatient stay,
except in the case of a transfer from another hospital (see section 212.530).
Arkansas Foundation for Medical Care Contact Information
In-state and out-of-state toll free for
inpatient reviews only
1-800-426-2234
General telephone contact, local or
long distance - Fort Smith
(479) 649-8501
.
1-877-650-2362
Fax for CHMS only
(479) 649- 0776
Fax
(479) 649-0799
Mailing address
Arkansas Foundation for Medical Care, Inc
PO Box 180001
Fort Smith, AR 72918-0001
Physical site location
2201 Brooken Hill Drive
Fort Smith, AR 72908
Office hours
8 30 a.m. until 5 00 p.m. (Central Time),
Monday through Friday, except holidays
15
Arkansas Medicaid Hospital Billing Tips
Outpatient Hospital Services
Outpatient hospital services are preventive, diagnostic, therapeutic, rehabilitative or
palliative services that:
A. Are furnished to outpatients and
B. Except in the case of nurse midwife services, are furnished by or under the
direction of a physician or dentist.
Coverage
Medicaid covers medically necessary outpatient services typically available in
hospitals.
For the purposes of reimbursement determination and benefit limitation, outpatient
hospital services are divided into four types of service:
A. Emergency services
B. Non-emergency services
C. Therapy and treatment services
D. Outpatient surgical procedures
Emergency Services
A. Emergency services are inpatient or outpatient hospital services that a prudent
layperson with an average knowledge of health and medicine would reasonably
believe are necessary to prevent death or serious impairment of health and
which, because of the danger to life or health, must be obtained at the most
accessible hospital available and equipped to furnish those services.
B. Emergency services comprise the following non-physician facility
accommodations and services.
1. Initial assessment to evaluate the patient’s complaint or presenting condition.
a. Assessment is included in the coverage of the basic emergency or nonemergency service.
b. If, following assessment, the patient is discharged or leaves the facility
without being treated for an emergent or non-emergent condition, only the
assessment and related medically necessary diagnostic services are
covered.
2. Treatment room and related non-physician services.
3. Outpatient hospital emergency supplies.
4. Outpatient hospital emergency drugs and injections.
C. Emergency services do not require prior authorization when deemed a true
emergency.
D. Emergency services do not require a primary care physician (PCP) referral when
deemed a true emergency.
16
Benefit Limit for Emergency Services
Emergency services are subject to retrospective review by the QIO; therefore, no
benefit limits are placed on emergency services. Special billing procedures are
required in order for emergency claims to bypass the benefit limitation audits. See
Section 272.400 of the Hospital provider manual for special billing instructions.
Non-Emergency Services
A. Non-emergency services in the emergency department and outpatient hospital
clinic services are not covered separately on the same date of service as an
inpatient admission.
B. Coverage of outpatient surgeries and treatment/therapy services include the
coverage of outpatient hospital clinic services (room) and basic non-emergency
services (room) in the emergency department that occur on the same date of
service.
C. See sections 172.100 and 172.200 of your provider manual for exceptions to the
PCP referral requirement.
The basic non-emergency outpatient facility service is provision of a
treatment/examination room with non-physician staffing and routine disposable
supplies.
A. Coverage of the basic non-emergency facility service is included in the coverage
of outpatient surgery and most treatment/therapy services.
B. Diagnostic lab, X-ray and machine tests are covered separately from the basic
non-emergency service.
C. Some services, such as observation bed or fetal monitoring, may be covered
separately when provided in conjunction with the basic non-emergency service.
Outpatient Assessment in the Emergency Department
Assessment does not require a PCP referral; however, the individual being assessed
must be enrolled with a PCP in order for the assessment to be covered.
A. If a Medicaid beneficiary is not already enrolled with a PCP when he or she
presents to the outpatient department, hospital staff may enroll the individual via
the Medicaid Voice Response System (VRS).
B. PCP enrollment on the same day as outpatient assessment in the emergency
department permits coverage of the assessment without PCP referral.
C. Medicaid pays the hospital an additional PCP enrollment fee as well.
17
Arkansas Medicaid Hospital Billing Tips
Benefit Limit for Outpatient Assessment in the Emergency Department
Outpatient assessment in the emergency department is included in the benefit limit
for non-emergency outpatient hospital services. See section 215.020 of the Hospital
provider manual for detailed information.
Emergency, Non-Emergency and Related Charges
National
Code
Local Code
Local Code Description
450*
Z0646
Emergency Room Coverage. Condition code 88
required.
459*
Z0647
Non-emergency Service Room Charge. This Service
Room Charge includes supplies, drugs and injections.
622*
Z0648
Outpatient Hospital Supplies - emergency only.
250*
Z0649
Outpatient Hospital drugs and injection; emergency only.
*Revenue code
18
Non-Emergency Charges
The following procedure codes may be billed in conjunction with procedure code
459* (Z0647) – “Other non-emergency service”, which includes room charge:
A. HCPCS Procedure Codes
9401094770
94642
96913
99199
J1600
J2290
J2790
J2910
J3420
J9000J9999
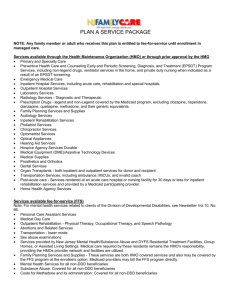
Medicaid Emergency Room Visits
Referral
Hospital Bills
Medicaid Pays
Referral is not
Required
Rev code 451
$15.00 Plus
Ancillary Charges
Rev code 459
$12.00 Plus
Ancillary Charges
No Drugs or
Supplies
Referral Required
450
Referral Not
Required
Enrollment Fee
622
250
Rev code 960
Service
Assess and Screen
You cannot bill if any form of
treatment
has already been provided.
Does not count as one of the
12 outpatient visits. Patients
under 21 are not limited to 12
visits.
Non -Emergency
After assessment treatment
was administered.
Counts as one of the 12
outpatient visits.
Patients under 21 are not
limited to 12 visits
$51.00 Plus
Ancillary Charges
Supplies
Drugs and Supplies
Paid
True Emergency
Does not count as one of the
12 outpatient visits.
$5.00 PCP
Enrollment Fee
Arkansas Medicaid reimburses
Hospitals a fee for enrolling
patients that do not have a
PCP. You can call the (PCP)
Enrollment Voice Response
System 1.800.805.1512.
Physician Bills
Medicaid Pays
T1015
$24.20
T1015 Modifier
U1
$31.90
99281
99282
99283
99284
99285
$22.00
$35.00
$53.90
$71.50
$83.75
Laboratory, Radiology and Machine Test Services
Laboratory and X-ray services are mandatory services in the Title XIX (Medicaid)
Program. The Arkansas Title XIX State Plan describes the services thus covered as:
19
Arkansas Medicaid Hospital Billing Tips
“Other lab and X-ray services when ordered and provided by a physician or under
the direction of a physician or other licensed practitioner of the healing arts within the
scope of his or her practice as defined by State law in the practitioner’s office or
outpatient hospital setting or by a certified independent lab that meets requirements
for participation in Title XVIII.”
A. Laboratory, radiology and machine test procedures are covered in conjunction
with each of the four categories of outpatient services listed in this manual.
B. Laboratory, radiology and machine test procedures are also covered in hospitals
as reference services for non-patients. Refer to the special billing procedures
that apply to reference diagnostic services for non-patients.
Benefit Limit in Outpatient Laboratory, Radiology and
Machine Test Procedures
Arkansas Medicaid limits payment for outpatient laboratory, radiology and machine
test procedures to a total of $500.00 per year per beneficiary aged 21 and older.
A. This yearly limit is based on the state fiscal year, July 1 through June 30.
B. This limitation applies to payments made to the following providers, individually
or in any combination: outpatient hospitals, independent laboratories, physicians,
osteopaths, podiatrists, certified nurse-midwives and nurse practitioners.
C. Requests for extensions of this benefit are considered for beneficiaries who
require supportive treatment for maintaining life.
D. Extension of this benefit is automatic for patients whose primary diagnosis for the
service furnished is in the following list:
1. Malignant neoplasm (ICD-9-CM code range 140.0 through 208.91)
2. HIV infection and AIDS (ICD-9-CM code 042)
3. Renal failure (ICD-9-CM code range 584 through 586)
E. Magnetic Resonance Imaging (MRI) is exempt from the $500.00 outpatient
laboratory and X-ray annual benefit limit. Medical necessity for each MRI must
be documented in the beneficiary’s medical record. Refer to Section 270.000 of
the Hospital provider manual for billing information.
F. Cardiac catheterization procedures are exempt from the $500.00 outpatient
laboratory and X-ray annual benefit limit. Medical necessity for each procedure
must be documented in the beneficiary’s medical record.
G. There are no benefit limits on outpatient laboratory, radiology and machine test
procedures for beneficiaries under age 21 in the Child Health Services (EPSDT)
Program, except for fetal non-stress test and fetal ultrasounds. See Section
215.041 of the Hospital provider manual.
Benefit Limits for Fetal Non-Stress Test and Fetal Ultrasound
A. Fetal echography (ultrasound) is limited to two (2) per pregnancy.
B. Fetal non-stress test is limited to two (2) per pregnancy.
C. Extension of benefits for these procedures will be considered for reasons of
medical necessity.
20
Observation Bed Status
Observation bed status is an outpatient designation. Coverage of hospital
observation services is contingent upon medical service providers' following
Arkansas Medicaid criteria regarding inpatient and outpatient status.
A. If a patient is expected to remain in the hospital for less than 24 consecutive
hours and this expectation is realized, the hospital and the physician should
consider the patient an outpatient; i.e., the patient is an outpatient unless the
physician has admitted him or her as an inpatient.
B. If the physician or hospital expects the patient to remain in the hospital for 24
hours or more, Medicaid deems the patient admitted at the time the patient’s
medical record indicates the existence of such an expectation, regardless of
whether the physician has formally admitted the patient.
C. Medicaid also deems a patient admitted to inpatient status at the time the patient
has remained in the hospital for 24 consecutive hours, even though the physician
or hospital may have had no prior expectation of a stay of that or greater
duration.
D. If a patient receives any outpatient services (including observation services) and
is subsequently admitted to inpatient status on the same date of service,
Medicaid's coverage of the inpatient service includes coverage of the outpatient
services.
E. Medicaid covers observation to perform external fetal monitoring of a patient in
suspected labor, if the hospital does not subsequently admit the patient to
inpatient status on the same date of service as the initiation of external fetal
monitoring.
Observation Bed Policy Illustration
The following table gives examples of appropriate billing for hospital services
involving patients in observation bed status. The billing instructions in the third and
fourth columns do not necessarily include all services for which the hospital may bill.
For instance, they do not state that you may bill for lab, X-ray, emergency room, etc.
The purpose of this table is to illustrate Arkansas Medicaid observation bed policy
and Medicaid criteria determining inpatient and outpatient status.
Observation Bed Billing Information
Use code 760* (Z1554) to bill for Observation Bed. One unit of service on the CMS1450 (UB-04) outpatient claim equals 1 hour of service. Medicaid will cover up to 8
hours of hospital observation per date of service.
When a physician admits a patient to observation subsequent to providing
emergency or non-emergency services in the emergency department, the hospital
may bill the observation bed code 760* (Z1554) and the appropriate procedure code
for emergency room 450* (Z0646) or non-emergency room 459* (Z0647). Condition
code 88 must be billed to indicate an emergency claim.
You may not bill 622* (Z0648) or 250* (Z0649):
A. Alone or in conjunction with only one another.
21
Arkansas Medicaid Hospital Billing Tips
B. With the non-emergency room procedure code 459* (Z0647).
C. With an outpatient surgical procedure.
D. Without code 450* (Z0646).
*Revenue code
OBSERVATION BED STATUS POLICY ILLUSTRATION
Patient is Admitted
to Observation
Patient is:
For Tuesday
Services, the
Hospital:
For Wednesday
Services, the
Hospital:
Tuesday, 3:00 PM
Still in Observation
Wednesday, 3:00 PM
May bill Medicaid for
up to 8 hours of
medically necessary
Observation Bed
Status.
Must admit the
patient to inpatient
status at 3:00 PM.
Tuesday, 3:00 PM
Discharged
Wednesday 12:00
PM (noon)
May bill Medicaid for
up to 8 hours of
medically necessary
Observation Bed
Status.
May bill Medicaid for
up to 8 hours of
medically necessary
Observation Bed
Status.
Tuesday, 3:00 PM
Discharged
Wednesday 4:00 PM
May bill Medicaid for
up to 8 hours of
medically necessary
Observation Bed
Status.
Appropriate level of
Initial Hospital Care
Tuesday, 3:00 PM,
after outpatient
surgery
Discharged
Wednesday 10:00
AM
Must bill Medicaid for
outpatient surgery.
May bill Medicaid for
up to 8 hours of
medically necessary
Observation Bed
Status.
Benefit Limit for Non-Emergency Services
A. Non-emergency outpatient hospital services are:
1. Non-emergency outpatient hospital and related physician services, and
2. Outpatient hospital treatment and therapy services and related physician
services.
B. Beneficiaries aged 21 and older are limited to a total of 12 non-emergency
outpatient hospital visits per state fiscal year, July 1 through June 30.
1. The outpatient hospital benefit limit includes outpatient hospital services
provided in an acute care/general hospital, a rehabilitative hospital or
both.
2. Treatment and therapy services are included in the non-emergency
outpatient hospital services limit of 12 visits per state fiscal year.
3. Services that Medicaid covers separately when furnished in conjunction
with one another and that occur during the same outpatient encounter
22
count against this benefit limit as only one non-emergency outpatient
hospital service.
C. Requests for extension of this benefit are considered for patients who require
supportive treatment for maintaining life.
D. Extension of this benefit is automatic for patients whose primary diagnosis for the
service furnished is in the following list:
1.
2.
3.
4.
Malignant neoplasm (ICD-9-CM code range 140.0 through 208.91)
HIV infection and AIDS (ICD-9-CM code 042)
Renal failure (ICD-9-CM code range 584 through 586)
Pregnancy (ICD-9-CM code range 630 through 677, with applicable 4th
and 5th digits; and diagnosis codes V22, V23 and V28, with applicable 4th
digits)
E. Beneficiaries under age 21 in the Child Health Services (EPSDT) Program are
not benefit-limited, except with respect to the services listed in section 215.021 of
the Hospital provider manual.
23
Arkansas Medicaid Hospital Billing Tips
Billing for UB04
Most Common Inpatient Types of Bills:
111 – Complete Claim
112 – First Interim Claim
113 – Interim Claim
114 – Last Interim Claim
Type of Bill Code Structure – Three Digit Number
First Digit – Indicates Type of Facility
Code
Description
1
Hospital
2
Skilled Nursing
3
Home Health
4
Christian Science Hospital
5
Christian Science Extended
6
Intermediate Care
7
Clinic
8
Special Facility
Second Digit – Indicates Bill Classification
Code
Description
1
Inpatient (including Medicare Part A)
2
Inpatient (Medicare Part B Only)
3
Outpatient
4
Outpatient – Other (Medicare Use Only)
4
Outpatient – Non-Patient (Medicaid & Medicare)
5
Intermediate Care Level I
6
Intermediate Care Level II
7
Intermediate Care Level III
8
Swing Beds
0
Outpatient – Emergency Services
24
Third Digit – Indicates Frequency
Code
Description
0
Non – Payment/Zero Claim
1
Admit thru discharge claim
2
Interim FIRST claim
3
Interim CONTINUING claim
4
Interim LAST claim
5
At charges only claim
6
Adjustment of prior claim
7
Replacement of prior claim
8
Void/Cancel of prior claim
9
Reserved for national assignment
Admit Source Codes
Code
Description
1
Physician Referral
2
Clinic Referral
3
HMO Referral
4
Transfer from a hospital (*Different facility)
5
Transfer from a skilled nursing facility
6
Transfer from another health care facility
7
Emergency Room
8
Court/Law Enforcement
9
Information Not Available
A
Transfer from a Critical Access Hospital
B
Transfer from another home health agency
C
Readmission to same home health agency
D
Transfer from hospital inpatient in the same facility resulting in a separate
claim to the payer
25
Arkansas Medicaid Hospital Billing Tips
Admit Source Codes (Newborn)
Code
Description
1
Normal Delivery
2
Premature Delivery
3
Sick Baby
4
Extramural Birth
9
Information not available
Patient Status Codes
Code
Description
01
Discharged to Home or Self Care
02
Discharged/transferred to another short-term facility
03
Discharged/transferred to Skilled Nursing Facility
04
Discharged/transferred to Intermediate Care Facility
05
Discharged/transferred to another type of institution
06
Discharged/transferred to home under care of organized home health service
organization
07
Left against medical advice
20
Expired
30
Still patient
43
Discharged/transferred to a federal health care facility
61
Discharged/transferred to hospital-based Medicare approved swing bed
62
Discharged/transferred to an inpatient rehabilitation facility (IRF) including
rehabilitation distinct part units of a hospital
63
Discharged/transferred to a Medicare certified long-term care hospital
(LTCH)
64
Discharged/transferred to a nursing facility certified under Medicaid but not
certified under Medicare
65
Discharged/transferred to a psychiatric hospital or psychiatric distinct part
unit of a hospital
26
Condition Codes
Condition Code crosswalk
Inpatient claims and some outpatient claims require condition codes when you bill for
facility services. The table below provides the required condition codes for both
paper and electronic billing:
Use
Paper Claims
Electronic Claims
Inpatient claims resulting from
EPSDT
80
A1
Inpatient claims for a woman who
delivered
AB
80
Inpatient claims for a newborn
AN
81
Inpatient claims not related to a birth
AX
82
Outpatient Emergency room claims
None/(TOB=101)
88 (TOB=131)
Semi-private room
38
38
Private room, medically necessary
39
39
Renal dialysis self-training
73
73
Renal dialysis – home
74
74
Billing clarification: Inpatient claim type S 10/5/07
Bill covered and non-covered days in fields 39 through 41 of the UB04 claim form. In
the Code column, enter 80 for covered days or 81 for non-covered days. In the Value
Code Amount column, enter total units billed to the left of the vertical dotted line and
enter two zeroes to the right of the vertical dotted line. If you do not enter this
information correctly, your claim will be denied and will have to be reprocessed
Formula for determining total days for which to bill
eOB: 007-Total days not equal to the difference between the “From” and “To”
Dates
A. Verify that the sum of Covered Days and Non-Covered Days equals “Thru” minus
the “From” date unless Patient Status code is 30. Then the Covered Days
equals the “Thru” date minus the “From” date plus one.
B. “Thru” date minus “From” date unless Patient Status code is 30. Then the
Covered Days equals the “Thru” date minus the “From” date plus one.
C. Both - If the admittance date equals the discharge date, the system allows for
one day of service.
27
Arkansas Medicaid Hospital Billing Tips
Formula:
“Thru Date” – “From Date” = “Number of Days”
Example:
For a date of service of 06/24/10 through 06/30/10, your
calculations would be:
30
- 24
6
If the Patient Status code is 30 or 31 and still a patient (add 1 day.) Patient Status
code 01 is Admit Thru Discharged; then the total is 6 days.
Timely Filing
A clean claim (i.e., a claim with no errors) must be submitted no later than 12
months from the date of service. The 12-month filing deadline applies to all
claims.
Providers cannot electronically transmit claims to HP Enterprise Services for
dates of service over 12 months old.
Timely filing of Medicare-Medicaid crossover claims is required.
If a provider bills Medicare within the 12-month Medicaid filing limit and
Medicare pays the claim after the 12 month filing limit, Medicaid will pay their
portion of the claim if the Medicare claim is submitted to HP Enterprise
Services within 6 months of the Medicare paid date.
Medicare crossover claims that do not crossover from Medicare to Medicaid
can be billed electronically on the Provider Electronic Solution (PES)
software.
28
Revenue Codes
Subcategory
Code
001
011x
Description
Total charge
Room and
board—private
(medical or
general)
012X
Room and
board—
semiprivate two
bed (medical or
general)
013X
Room and
board—
semiprivate—
three and four
beds
014X
Room and
board—private
(deluxe)
Last
Digit
Description
Standard Abbreviation
0
1
2
3
4
5
6
7
8
9
0
1
2
3
4
5
6
7
8
9
0
1
2
3
4
5
6
7
8
9
0
1
2
3
4
5
6
7
8
9
General classification
Medical/surgical/gyn
OB
Pediatric
Psychiatric
Hospice
Detoxification
Oncology
Rehabilitation
Other
General classification
Medical/surgical/gyn
OB
Pediatric
Psychiatric
Hospice
Detoxification
Oncology
Rehabilitation
Other
General classification
Medical surgical/gyn
OB
Pediatric
Psychiatric
Hospice
Detoxification
Oncology
Rehabilitation
Other
General classification
Medical surgical/gyn
OB
Pediatric
Psychiatric
Hospice
Detoxification
Oncology
Rehabilitation
Other
Room board/PVT
Med-SUR-GY/PVT
OB/PVT
Peds/PVT
Psych/PVT
Hospice/PVT
Detox/PVT
Oncology/PVT
Rehab/PVT
Other/PVT
Room Board//Semi
Med-Sur-Gy/2Bed
OB/2Bed
Peds/2Bed
Pstay/2Bed
Hospice/2Bed
Detox/2Bed
Oncology/2Bed
Rehab/2Bed
Other/2Bed
Room-Board/3and4Bed
Med-Sur-Gy/3and4Bed
OB/3and4Bed
Peds/3and4Bed
Psych/3and4Bed
Hospice/3and4Bed
Detox/3and4Bed
Oncology/3and4Bed
Rehab/3and4Bed
Other/3and4Bed
Room-Board/PVT/DLX
Med-Sur-Gy/DLX
OB/DLX
Peds/DLX
Psych/DLX
Hospice/DLX
Detox/DLX
Oncology/DLX
Rehab/DLX
Other/DLX
29
Arkansas Medicaid Hospital Billing Tips
Subcategory
Code
015X
Description
Room and board
ward (medical or
general)
016X
Room and
board—other
017X
Nursery
018X
Leave of absence
019X
Subacute care
020X
Intensive care
Last
Digit
0
1
2
3
4
5
6
7
8
9
0
4
7
9
0
1
2
3
4
9
0
1
2
3
4
5
9
0
1
2
3
4
9
0
1
2
3
4
6
7
8
9
Description
General classification
Medical surgical/gyn
OB
Pediatric
Psychiatric
Hospice
Detoxification
Oncology
Rehabilitation
General Classification
General classification
Sterile environment
Self care
Other
General classification
Newborn – Level I
Newborn – Level II
Newborn – Level III
Newborn – Level IV
Other
General classification
Reserved
Patient convenience
Therapeutic leave
ICF/MR—any reason
Nursing home (for
hospitalization)
Other leave of absence
General classification
Subacute care – Level I
Subacute care – Level II
Subacute care – Level III
Subacute care – Level IV
Other subacute care
General classification
Surgical
Medical
Pediatric
Psychiatric
Intermediate ICU
Burn care
Trauma
Other intensive care
Standard Abbreviation
Room-Board/PVT/Ward
Med-Sur-Gy/Ward
OB/Ward
Peds/Ward
Psych/Ward
Hospice/Ward
Detox/Ward
Oncology/Ward
Rehab/Ward
Other/Ward
RandB
RandB/Sterile
RandB/Self
RandB/Other
Nursery
Nursery/Level I
Nursery/Level II
Nursery/Level III
Nursery/Level IV
Nursery/Other
Leave of Absence or LOA
LOA/Pt Conv
LOA/Therapeutic
LOA/ICF/MR
LOA/Nurs Home
LOA/Other
Subacute
Subacute/LevelI
Subacute/Level II
Subacute/Level III
Subacute/Level IV
Subacute/Other
Intensive Care or ICU
ICU/Surgical
ICU/Medical
ICU/Peds
ICU/Stay
ICU/Intermediate
ICU/Burn Care
ICU/Trauma
ICU/Other
30
Subcategory
Code
021X
Description
Coronary care
022X
Special charges
023X
Incremental
nursing charge
rate
024X
All-inclusive
ancillary
025X
Pharmacy (also
see 063X, an
extension of
025X)
026X
IV therapy
027X
Medical/surgical
supplies
Last
Digit
0
1
2
3
4
9
0
1
2
3
4
9
0
1
2
3
4
5
0
1
2
3
9
0
1
2
3
4
5
0
1
2
3
4
9
0
1
2
3
4
5
6
7
8
9
Description
General classification
Myocardial infarction
Pulmonary care
Heart transplant
Intermediate CCU
Other coronary care
General classification
Admission charge
Technical support charge
UR service charge
Late discharge, medically
necessary
Other special charges
General classification
Nursery
OB
ICU
CCU
Hospice
General classification
Basic
Comprehensive
Specialty
Other all-inclusive ancillary
General classification
Generic drugs
Nongeneric drugs
Take hospice drugs
Drugs incident to other
diagnostic services
Drugs incident to radiology
General classification
Infusion pump
IV therapy/pharmacy svcs
IV therapy/drug/supply
delivery
IV therapy/supplies
Other IV therapy
General classification
Nonsterile supply
Sterile supply
Take-home supplies
Prosthetic/orthotic devices
Pacemaker
Intraocular lens
Oxygen—take home
Other implants
Other supplies/devices
Standard Abbreviation
Coronary Care or CCU
CCU/Myo Infarc
CCU/Pulmonary
CCU/Transplant
CCU/Intermediate
CCU/Other
Special Charges
Admit Charge
Tech Suppt Chg
UR Charge
Late Disch/Med Nec
Other Spec Chg
Nursing Increm
Nur Incr/Nursery
Nur Incr/OB
Nur Incr/ICU
Nur Incr/CCU
Nur Incr/Hospice
All Incl Ancil
All Incl Basic
All Incl Comp
All Incl Special
All Incl Ancil/Other
Pharmacy
Drugs/Generic
Drugs/Non-Generic
Drugs/Take Home
Drugs/Incident Odx
Drugs/Incident Rad
IV Therapy
IV Ther/Infsn Pump
IV Ther/Pharm/Svc
IV Ther/Drug/Supply Delv
IV Ther/Supplies
IV Therapy/Other
Med-Sur Supplies
Non-Ster Supply
Sterile Supply
Take Home Supply
Prosth/Orth Dev
Pace Maker
Intra Oc Lens
O2 Take Home
Supply/Implants
Supply/Other
31
Arkansas Medicaid Hospital Billing Tips
Subcategory
Code
028X
Description
Oncology
029X
Durable
medical
equipment
(other than
renal)
030X
Laboratory
031X
Laboratory
pathological
032X
Radiology—
diagnostic
033X
Radiology—
therapeutic
and/or
chemotherapy
administration
Last
Digit
0
9
0
1
2
3
4
9
0
1
2
3
4
5
6
7
9
0
1
2
4
9
0
1
2
3
4
9
0
1
2
3
5
034X
Nuclear
medicine
035X
CT scan
9
0
1
2
9
0
1
2
9
Description
General classification
Other oncology
General classification
Rental
Purchase of new DME
Purchase of used DME
Supplies/drugs for DME
effectiveness (home health
agency only)
Other equipment
General classification
Chemistry
Immunology
Renal patient (home)
Nonroutine dialysis
Hematology
Bacteriology and
microbiology
Urology
Other laboratory
General classification
Cytology
Histology
Biopsy
Other laboratory pathological
General classification
Angiocardiography
Arthrography
Arteriography
Chest X-ray
Other radiology—diagnostic
General classification
Chemotherapy
administration—injected
Chemotherapy
administration—oral
Radiation therapy
Chemotherapy
administration—IV
Other radiology—therapeutic
General classification
Diagnostic
Therapeutic
Other nuclear medicine
General classification
Head scan
Body scan
Other CT scans
Standard Abbreviation
Oncology
Oncology/Other
Med Equip/Durab
Med Equip/Rent
Med Equip/New
Med Equip/Used
Med Equip/Supplies/Drugs
Med Equip/Other
Laboratory or (Lab)
Lab/Chemistry
Lab/Immunology
Lab/Renal Home
Lab/Nr Dialysis
Lab/Hematology
Lab/Bact-Micro
Lab/Urology
Lab/Other
Pathology Lab
Pathol/Cytology
Pathol/Hystol
Pathol/Biopsy
Pathol/Other
DX X-Ray
DX X-Ray/Angio
DX X-Ray/Arth
DX X-ray/Arter
DX X-ray/Chest
DX X-ray/Other
RX X-Ray
Chemother/Inj
Chemother/Oral
Radiation RX
Chemotherp-IV
RX X-ray/Other
Nuclear Medicine
Nuc Med/DX
Nuc Med/RX
Nuc Med/Other
CT Scan
CT Scan/Head
CT Scan/Body
CT Scan/Other
32
Subcategory
Code
036X
037X
Description
Operating room
services
Anesthesia
Last
Digit
0
1
2
7
9
0
1
2
038X
Blood
039X
Blood and blood
component
administration,
processing and
storage
Other imaging
services
040X
041X
Respiratory
services
042X
Physical therapy
4
9
0
1
2
3
4
5
6
7
9
0
1
9
0
1
2
3
4
9
0
2
3
9
0
1
2
3
4
9
Description
General classification
Minor surgery
Organ transplant other than
kidney
Kidney transplant
Other operating room svcs
General classification
Anesthesia incident to
radiology
Anesthesia incident to other
diagnostic services
Acupuncture
Other anesthesia
General classification
Packed red cells
Whole blood
Plasma
Platelets
Leucocytes
Other components
Other derivatives
(cryopricipitates)
Other blood
General classification
Administration (e.g.,
transfusions)
Other blood storage and
processing
General classification
Diagnostic mammography
Ultrasound
Screening mammography
Position emission
tomography
Other imaging services
General classification
Inhalation services
Hyperbaric oxygen therapy
Other respiratory services
General classification
Visit charge
Hourly charge
Group rate
Evaluation or reevaluation
Other physical therapy
Standard Abbreviation
OR Services
OR/Minor
OR/Organ Trans
OR/Kidney Trans
OR/Other
Anesthesia
Anesthe/Incident Rad
Anesthe/Incident Other DX
Anesthe/Acupunc
Anesthe/Other
Blood
Blood/Pkd Redt
Blood/Whole
Blood/Plasma
Blood/Platelets
Blood/Leucocytes
Blood/Components
Blood/Derivatives
Blood/Other
Blood/Stor – Proc
Blood/Admin
Blood/Other Stor
Image Service
Diag Mammography
Ultra Sound
Scrn Mammography
Pet Scan
Other Imag Svs
Respiratory Svc
InhalationSvc
Hyperaric O2
Other Respir Svs
Physical Therp
Phys Therp/Visit
Phys Therp/Hour
Phys Therp/Group
Phys Therp/Eval
Other Phys Therp
33
Arkansas Medicaid Hospital Billing Tips
Subcategory
Code
043X
Description
Occupational
therapy
044X
Speech-language
pathology
045X
Emergency room
Last
Digit
0
1
2
3
4
9
0
1
2
3
4
9
Description
General classification
Visit charge
Hourly charge
Group rate
Evaluation or reevaluation
Other occupational therapy
General classification
Visit charge
Hourly charge
Group rate
Evaluation or reevaluation
Other speech-language
pathology
General classification
EMTALA emergency
medical screening services
ER beyond EMTALA
screening
Urgent care
Other emergency room
General classification
Other pulmonary function
General classification
Diagnostic
Treatment
Other audiology
General classification
Cardiac cath lab
Stress test
Echocardiology
Other cardiology
General classification
Other ambulatory surgical
care
Standard Abbreviation
Occupation Ther
Occup Therp/Visit
Occup Therp/Hour
Occup Therp/Group
Occup Therp/Eval
Other Occup/Ther
Speech Pathol
Speech Path/Visit
Speech Path/Hour
Speech Path/Group
Speech Path/Eval
Other Speech Pat
0
General classification
Outpatient Svc
9
0
1
2
3
4
5
6
7
9
Other outpatient service
General classification
Chronic pain center
Dental clinic
Psychiatric clinic
OB-GYN clinic
Pediatric clinic
Urgent care clinic
Family practice clinic
Other clinic
Outpatient/Other
Clinic
Chronic Pain Cl
Dental Clinic
Psych Clinic
OB-GYN Clinic
Peds Clinic
Urgent Clinic
Family Clinic
Other Clinic
0
1
2
046X
047X
Pulmonary
function
Audiology
048X
Cardiology
049X
Ambulatory
surgical care
050X
Outpatient
services
051X
Clinic
6
9
0
9
0
1
2
9
0
1
2
3
9
0
9
Emerg Room
ER/EMTALA
ER/Beyond EMTALA
Urgent Care
Other Emer Room
Pulmonary Func
Other Pulmon Func
Audiology
Audiology/DX
Audiology/RX
Other Audiology
Cardiology
Cardiac Cath Lab
Stress Test
Echocardiology
Other Cardiology
Ambul Surg
Other Ambl Surg
34
Subcategory
Code
052X
Description
Free-standing
clinic
053X
Osteopathic
services
054X
Ambulance
Last
Digit
0
1
2
3
6
9
0
1
9
0
1
2
3
4
5
6
7
8
055X
Skilled nursing
056X
Medical social
services
057X
Home health—
Home health aide
058X
Home health—
other visits
059X
Home health—
Units of service
Home health—
Oxygen
060X
9
0
1
2
9
0
1
2
9
0
1
2
9
0
1
2
3
9
0
9
0
1
2
3
4
9
Description
General classification
Rural health-clinic
Rural health-home
Family practice clinic
Urgent care clinic
Other free-standing clinic
General classification
Osteopathic therapy
Other osteopathic services
General classification
Supplies
Medical transport
Heart mobile
Oxygen
Air ambulance
Neonatal ambulance
services
Pharmacy
Telephone transmission
EKG
Other ambulance
General classification
Visit charge
Hourly charge
Other skilled nursing
General classification
Visit charge
Hourly charge
Other med social service
General classification
Visit charge
Hourly charge
Other home health aide
General classification
Visit charge
Hourly charge
Assessment
Other home health visit
General classification
Home health other units
General classification
Oxygen—
state/equip/suppl/or cont
Oxygen—
state/equip/suppl/under 1
LPM
Oxygen—state/equip/over 4
LPM
Oxygen—portable add-on
Other oxygen
Standard Abbreviation
Freestand Clinic
Rural/Clinic
Rural/Home
FR/STD Family Clinic
FR/STD Urgent Clinic
Other FR/STD Clinic
Osteopath Svs
Osteopath RX
Other Osteopath
Ambulance
Ambul/Supply
Ambul/Med Trans
Ambul/Heart Mobl
Ambul/Oxy
Air Ambulance
Ambul/Neonat
Ambul/Pharmacy
Ambul/Telephone EKG
Other Ambulance
Skilled Nursing
Skilled Nurs/Visit
Skilled Nurs/Hour
Skilled nurs/Other
Med Social Svs
Med Soc Servs/Visit
Med Soc Serv/Hour
Med Soc Serv/Other
Aide/Home Health
Aide/Home Hlth/Visit
Aide/Home Hlth/Hour
Aide/Home Hlth/Other
Visit/Home Health
Visit/Home Hlth/Visit
Visit/Home Hlth/Hour
Visit/Home Hlth/Assess
Visit/Home Hlth/Other
Unit/Home Health
Unit/Home Hlth/Other
O2/Home Health
O2/Stat Equip/Suppl/Cont
O2/Stat Equip/Under 1 LPM
O2/Stat Equip/Over 4 LPM
O2/Portable Add-on
O2—Other
35
Arkansas Medicaid Hospital Billing Tips
Subcategory
Code
061X
062X
063X
Description
Magnetic
resonance
technology
(MRT)
Medicare/surgical
supplies—
extension of
027X
Pharmacy—
extension of
025X
Last
Digit
0
1
2
3
4
5
6
7
8
9
1
2
3
4
0
1
2
3
4
5
6
064X
Home IV therapy
services
7
0
1
2
3
4
5
6
7
8
9
Description
General admission
MRI—brain (including
brainstem)
MRI—spinal cord (including
spine)
Reserved
MRI—other
MRA—head and neck
MRA—lower extremities
Reserved
MRA—other
Other MRT
Supplies incident to
radiology
Supplies incident to other
diagnostic services
Surgical dressings
FDA investigational devices
Reserved (effective 1/1/98)
Single source drug
Multiple source drug
Restrictive prescription
Erythropoietin (EPO) less
than 10,000 units
Erythropoietin (EPO) 10,000
or more units
Drugs requiring detailed
coding
Self-administrable drugs
General classification
Nonroutine nursing, central
line
IV site care, central line
IV start/change, peripheral
line
Nonroutine nursing,
peripheral line
Training patient/caregiver.
central line
Training, disabled patient,
central line
Training, patient/caregiver,
peripheral line
Training, disabled patient,
peripheral line
Other IV therapy services
Standard Abbreviation
MRT
MRI – Brain
MRI – Spine
MRI – Other
MRA – Head and Neck
MRA – Lower Ext
MRA – Other
MRT – Other
Med-Sur Supp/Incdnt Rad
Med-Sur Supp/Incdnt ODX
Surg Dressing
FDA Invest Device
Drug/Single
Drug/Mult
Drug/Rstr
Drug/EPO<10,000 Units
Drug/EPO>10,000 Units
Drugs/Detail Code
Drugs/Self Admin
IV Therapy Svc
Non Rt Nursing/Central
IV Site Care/Central
IV Strt/Chng/Periphal
Nonrt Nursing/Periphrl
Trng Pt/Caregvr/Centrl
Trng Dsblpt/Central
Trng/Pt/Cargvr/Periphrl
Trng/Dsblpat/Periphrl
Other IV Therapy Svc
36
Subcategory
Code
065X
Description
Hospice service
Last
Digit
0
1
2
3
4
5
6
7
8
066X
Respite care
067X
Outpatient
special residence
charges
068X
Trauma response
069X
070X
Not assigned
Cast room
071X
Recovery room
072X
Labor
room/delivery
073X
EKG/ECG
(electrocardiogram)
074X
EEG
(electroencephalogram)
9
0
1
2
3
9
0
1
2
9
0
1
2
3
4
9
0
9
0
9
0
1
2
3
4
9
0
1
2
9
0
9
Description
General classification
Routine home care
Continuous home care
Reserved
Reserved
Inpatient respite care
General inpatient care
(nonrespite)
Physician services
Hospice room and board—
nursing facility
Other hospice service
General classification
Hourly charge/nursing
Hourly charge/aide/
homemaker/companion
Daily respite charge
Other respite care
General classification
Hospital based
Contracted
Other special residence
charge
Not used
Level I
Level II
Level III
Level IV
Other trauma response
General classification
Other cast room
General classification
Other recovery room
General classification
Labor
Delivery
Circumcision
Birthing center
Other labor room/delivery
General classification
Holter monitor
Telemetry
Other EKG/ECG
General classification
Other EEG
Standard Abbreviation
Hospice
Hospice/Rtn Home
Hospice/Ctns Home
Hospice/IP Respite
Hospice/IP Non-Respite
Hospice/Physician
Hospice/R&B/Nurs Fac
Hospice/Other
Respite Care
Respite/Nurse
Respite/Aide/Hmemkr/Comp
Respite Daily
Respite Other
OP Spec Res
OP Spec Res/Hosp Based
OP Spec Res/Contracted
OP Spec Res/Other
Trauma Level I
Trauma Level II
Trauma Level III
Trauma Level IV
Trauma Other
Cast Room
Other Cast Room
Recovery Room
Other Recovery Rm
Deliveroom/Labor
Labor
Delivery Room
Circumcision
Birthing Center
Other/Deliv-Labor
EKG/ECG
Holter Mont
Telemetry
Other EKG/ECG
EEG
Other EEG
37
Arkansas Medicaid Hospital Billing Tips
Subcategory
Code
075X
076X
Description
Gastro-intestinal
services
Treatment/observ
ation room
Last
Digit
0
9
0
1
2
9
077X
Preventive care
services
0
1
9
078X
Telemedicine
079X
Lithotripsy
080X
Inpatient renal
dialysis
0
9
0
9
0
1
2
3
4
081X
Acquisition of
body components
082X
Hemodialysis—
outpatient or
home
083X
Peritoneal
dialysis—
outpatient or
home
9
0
1
2
3
4
9
0
1
2
3
4
5
0
1
2
3
4
5
9
Description
General classification
Other gastro-intestinal
General classification
Treatment room
Observation room
Other treatment/observation
room
General classification
Vaccine administration
Other preventive care
services
General classification
Other telemedicine
General classification
Other lithotripsy
General classification
Inpatient hemodialysis
Inpatient peritoneal (noncapd)
Inpatient continuous
ambulatory peritoneal
dialysis (CAPD)
Inpatient continuous cycling
peritoneal dialysis (CCPD)
Other inpatient dialysis
General classification
Living donor
Cadaver donor
Unknown donor
Unsuccessful organ
search—donor bank charges
Other donor
General classification
Hemodialysis/composite or
other rate
Home supplies
Home equipment
Maintenance/100%
Support services
General classification
Peritoneal/composite or
other rate
Home supplies
Home equipment
Maintenance100%
Support services
Other outpatient peritoneal
dialysis
Standard Abbreviation
Gastr-Inst Svs
Other Gastro-Ints
Treatment/Observation Rm
Treatment Rm
Observation Rm
Other Treat/Observ Rm
Prevent Care Svs
Vaccine Admin
Other Prevent
Telemedicine
Telemedicine/Other
Lithotripsy
Lithotripsy/Other
Renal Dialysis
Dialy/Inpt
Disly/Inpt/Per
Daily/Inpt/Capd
Daily/Inpt/CCPD
daily/Inpt/Other
Organ Acquisit
Living Donor
Cadaver Donor
Unknown Donor
Unsuccessful Search
Other Donor
Hemo/OP or Home
Hemo/Composite
Hemo/Home/Suppl
Hemo/Home/Equip
Hemo/Home/100%
Hemo/Home/Supserv
Peritoneal/OP or Home
Pertnl/Composite
Pertnl/Home/Suppl
Pertnl/Home/Equip
Pertnl/Home/100%
Pertnl/Home/Supserv
Perntl/Home/Other
38
Subcategory
Code
084X
085X
086X
087X
088X
089X
090X
091X
Description
Continuous
ambulatory
peritoneal
dialysis
(CAPD)—
outpatient or
home
Last
Digit
0
1
Description
General classification
CAPD/composite or other
rate
2
Home supplies
3
Home equipment
4
Maintenance 100%
5
Support services
9
Other outpatient CAPD
Continuous
0
General classification
cycling peritoneal 1
CCPD/composite or other
dialysis
rate
(CCPD)—
2
Home supplies
outpatient or
3
Home equipment
home
4
Maintenance 100%
5
Support services
9
Other outpatient CCPD
Reserved for dialysis (national assignment)
Reserved for dialysis (national assignment)
Miscellaneous
0
General classification
dialysis
1
Ultrafiltration
2
Home dialysis aid visit
9
Other miscellaneous dialysis
Reserved for national assignment
Psychiatric/psych 0
General classification
ological
1
Electroshock treatment
treatments
2
Milieu therapy
3
Play therapy
4
Activity therapy
9
Other psychiatric/
psychological treatment
Psychiatric/psych 0
General classification
ological services
1
Rehabilitation
2
Partial hospitalization—less
intensive
3
Partial hospitalization—
intensive
4
Individual therapy
5
Group therapy
6
Family therapy
7
Biofeedback
8
Testing
9
Other psychiatric/
psychological service
Standard Abbreviation
CAPD/OP or Home
CAPD/Composite
CAPD/Home/Suppl
CAPD/Home/Equip
CAPD/Home/100%
CAPD/Home/Supserv
CAPD/Home/Other
CCPD/OP or Home
CCPD/Composite
CCPD/Home/Suppl
CCPD/Home/Equip
CCPD/Home/100%
CCPD/Home/Supserv
CCPD/Home/Other
Dialy/Misc
Dialy/Ultrafilt
Home Dialysis Aid Visit
Daily/Misc/Other
Psych Treatment
ElectroShock
Milieu Therapy
Play Therapy
Activity Therapy
Other Psych RX
Psych Services
Psych/Rehab
Psych/Partial Hosp
Psych/Partial Intensive
Psych/Indiv RX
Psych/Group RX
Psych/Family RX
Psych/Biofeed
Psych/Testing
Psych/Other
39
Arkansas Medicaid Hospital Billing Tips
Subcategory
Code
092X
Description
Other diagnostic
services
093X
Medical
rehabilitation day
program
Other therapeutic
services (see
also 095X, an
extension of
094X)
094X
Last
Digit
0
1
2
3
4
5
9
1
2
0
1
2
3
4
5
6
7
095X
096X
097X
Other therapeutic
services—
extension of
094X
Professional fees
(see also 097X
and 098X)
Professional fees
(extension of
096X)
9
0
1
2
0
1
2
3
4
9
1
2
3
4
5
6
7
8
9
Description
General classification
Peripheral vascular lab
Electromyelgram
Pap smear
Allergy test
Pregnancy test
Other diagnostic service
Half day
Full day
Standard Abbreviation
Other DX Svs
Peri Vascul Lab
Emg
Pap Smear
Allergy Test
Preg Test
Additional DX Svs
Half Day
Full Day
General classification
Recreational therapy
Education/training
Cardiac rehabilitation
Drug rehabilitation
Alcohol rehabilitation
Complex medical
equipment—routine
Complex medical
equipment—ancillary
Other therapeutic services
Reserved
Athletic training
Kinesiotherapy
Other RX Svs
Recreation RX
Education/Training
Cardiac Rehab
Drug Rehab
Alcohol Rehab
Cmplx Med Equip-Rout
General classification
Psychiatric
Opthalmology
Anesthesiologist (MD)
Anesthetist (CRNA)
Other professional fees
Laboratory
Radiology—diagnostic
Radiology—therapeutic
Radiology—nuclear
medicine
Operating room
Respiratory therapy
Physical therapy
Occupational therapy
Speech pathology
Pro Fee
Pro Fee/Psych
Pro Fee/Eye
Pro Fee/Anes MD
Pro Fee/Anes CRNA
Other Pro Fee
Pro Fee/Lab
Pro Fee/Rad/Dx
Pro Fee/Rad/Rx
Pro Fee/Nuc Med
Cmplx Med Equip-Anc
Additional RX Svs
Athletic Training
Kinesiotherapy
Pro Fee/Or
Pro Fee/Respir
Pro Fee/Physi
Pro Fee/Occupa
Pro Fee/Speech
40
Subcategory
Code
098X
Description
Professional fees
(extension of
096X and 097X)
Last
Digit
1
2
3
4
5
6
7
8
9
0
1
2
3
4
5
6
7
8
9
Description
Emergency room
Outpatient services
Clinic
Medical social services
EKG
EEG
Hospital visit
Consultation
Private duty nurse
099X
Patient
General classification
convenience
Cafeteria/guest tray
items
Private linen service
Telephone/telegraph
TV/radio
Non-patient room rentals
Late discharge charge
Admission kits
Beauty shop/barber
Other patient convenience
items
100X to 209X Reserved for national assignment
210X
Patient
0
General classification
convenience
1
Acupuncture
items
2
Acupressure
3
Massage
4
Reflexology
5
Biofeedback
6
Hypnosis
9
Other alternative therapy
services
211X to 309X Reserved for national assignment
310X
Adult care
0
Not used
1
Adult day care, medical and
social—hourly
2
Adult day care, social—hourly
3
Adult day care, medical and
social—daily
4
Adult day care, social—daily
5
Adult foster care—daily
9
Other adult care
Standard Abbreviation
Pro Fee/ER
Pro Fee/Outpt
Pro Fee/Clinic
Pro Fee/Soc Svc
Pro Fee/EKG
Pro Fee/EEG
Pro Fee/Hos Vis
Pro Fee/Consult
Pro Fee/Pvt Nurse
Pt Convenience
Cafeteria
Linen
Telephone
TV/Radio
Non-Pt Room Rent
Late Discharge
Admit Kit
Barber/beauty
Pt Convenience/Oth
Alttherapy
Acupuncture
Acupressure
Massage
Reflexology
Biofeedback
Hypnosis
Other Alttherapy
Adult Med/Soc Hr
Adult Soc Hr
Adult Med/Soc Day
Adult Soc Day
Adult Foster Day
Other Adult
41
Arkansas Medicaid Hospital Billing Tips
Hospital Billing Instructions – Paper Only
Field #
Field name
Description
1.
(blank)
Inpatient and Outpatient: Enter the provider’s name, city,
state, ZIP code and telephone number.
2.
(blank)
Unassigned data field.
3a.
PAT CNTL #
Inpatient and Outpatient: The provider may use this
optional field for accounting purposes. It appears on the
RA beside the letters “MRN.” Up to 16 alphanumeric
characters are accepted.
3b.
MED REC #
Inpatient and Outpatient: Required. Enter up to
15 alphanumeric characters.
4.
TYPE OF BILL
Inpatient and Outpatient: See the UB-04 manual. Fourdigit code with a leading zero that indicates the type of
bill.
5.
FED TAX NO
Not required.
6.
STATEMENT
COVERS PERIOD
Enter the covered beginning and ending service dates.
Format: MMDDYY.
Inpatient: Enter the dates of the first and last covered
days in the FROM and THROUGH fields.
The FROM and THROUGH dates cannot span the
State’s fiscal year end (June 30) or the provider’s fiscal
year end.
To file correctly for covered inpatient days that span a
fiscal year end:
1. Submit one interim claim (a first claim or a continuing
claim, as applicable) on which the THROUGH date is
the last day of the fiscal year that ended during the
stay.
On a first claim or a continuing claim, the patient
status code in field 17 must indicate that the
beneficiary is still a patient on the indicated
THROUGH date.
2. Submit a second interim claim (a continuing claim or a
last claim, as applicable) on which the FROM date is
the first day of the new fiscal year.
When the discharge date is the first day of the
provider’s fiscal year or the state’s fiscal year, only
one (bill type: admission through discharge) claim is
necessary, because Medicaid does not reimburse a
hospital for a discharge day unless the discharge day
is also the first covered day of the inpatient stay.
When an inpatient is discharged on the same date he
or she is admitted, the day is covered when the TYPE
OF BILL code indicates that the claim is for admission
through discharge, the STAT (patient status) code
42
Field #
Field name
Description
indicates discharge or transfer and the FROM and
THROUGH dates are identical.
Outpatient: To bill on a single claim for outpatient
services occurring on multiple dates, enter the beginning
and ending service dates in the FROM and THROUGH
fields of this field.
The dates in this locator must fall within the same
fiscal year – the state’s fiscal year and the hospital’s
fiscal year.
When billing for multiple dates of service on a single
claim, a date of service is required in field 45 for each
HCPCS code in field 44 and/or each revenue code in
field 42.
7.
(blank)
Unassigned data field.
8a.
PATIENT NAME
Inpatient and Outpatient: Enter the patient’s last name
and first name. Middle initial is optional.
8b.
(blank)
Not required.
9.
PATIENT
ADDRESS
Inpatient and Outpatient: Enter the patient’s full mailing
address. Optional.
10.
BIRTH DATE
Inpatient and Outpatient: Enter the patient’s date of birth.
Format: MMDDYYYY.
11.
SEX
Inpatient and Outpatient: Enter M for male, F for female
or U for unknown.
12.
ADMISSION DATE
Inpatient: Enter the inpatient admission date. Format:
MMDDYY.
Outpatient: Not required.
13.
ADMISSION HR
Inpatient and Outpatient: Enter the national code that
corresponds to the hour during which the patient was
admitted for inpatient care.
14.
ADMISSION TYPE
Inpatient: Enter the code from the Uniform Billing Manual
that indicates the priority of this inpatient admission.
Outpatient: Not required.
15.
ADMISSION SRC
Inpatient and Outpatient: Admission source. Required.
Code 1, 2, 3 or 4 is required when the code in field 14 is
4.
16.
DHR
Inpatient: See the UB-04 Manual. Required except for
type of bill 021x. Enter the hour the patient was
discharged from inpatient care.
17.
STAT
Inpatient: Enter the national code indicating the patient’s
status on the Statement Covers Period THROUGH date
(field 6).
Outpatient: Not applicable.
43
Arkansas Medicaid Hospital Billing Tips
Field #
Field name
Description
18.-28.
CONDITION
CODES
Inpatient and Outpatient: Required when applicable.
See the UB-04 Manual for requirements and for the
codes used to identify conditions or events relating to this
bill.
29.
ACDT STATE
Not required.
30.
(blank)
Unassigned data field.
31.-34.
OCCURRENCE
CODES AND
DATES
Inpatient and Outpatient: Required when applicable.
See the UB-04 Manual.
35.-36.
OCCURRENCE
SPAN CODES AND
DATES
Inpatient: Enter the dates of the first and last days
approved, per the facility’s PSRO/UR plan, in the FROM
and THROUGH fields. See the UB-04 Manual. Format:
MMDDYY.
Outpatient: See the UB-04 Manual.
37.
(blank)
Unassigned data field.
38.
Responsible Party
Name and Address
See the UB-04 Manual.
39.
VALUE CODES
Outpatient: Not required.
Inpatient:
a.
b.
CODE
Enter 80.
AMOUNT
Enter number of covered days.
CODE
Enter 81.
AMOUNT
Enter number of non-covered days.
40.
VALUE CODES
Not required.
41.
VALUE CODES
Not required.
42.
REV CD
Inpatient and Outpatient: See the UB-04 Manual.
43.
DESCRIPTION
See the UB-04 Manual.
44.
HCPCS/RATE/HIPP
S CODE
See the UB-04 Manual.
45.
SERV DATE
Inpatient: Not applicable.
Outpatient: Date format: MMDDYY.
46.
SERV UNITS
Comply with the UB-04 Manual’s instructions when
applicable to Medicaid.
47.
TOTAL CHARGES
Comply with the UB-04 Manual’s instructions when
applicable to Medicaid.
48.
NON-COVERED
CHARGES
See the UB-04 Manual, line item “Total” under
“Reporting.”
49.
(blank)
Unassigned data field.
44
Field #
Field name
Description
50.
PAYER NAME
Line A is required. See the UB-04 for additional
regulations.
51.
HEALTH PLAN ID
Not required.
52.
REL INFO
Required when applicable. See the UB-04 Manual.
53.
ASG BEN
Required. See “Notes” at field 53 in the UB-04 Manual.
54.
PRIOR PAYMENTS
Inpatient and Outpatient: Enter the total of payments
previously received on this claim. Do not include amounts
previously paid by Medicaid. * Do not include in this total
the automatically deducted Medicaid or ARKids First-B
co-payments.
55.
EST AMOUNT DUE
Situational. See the UB-04 Manual.
56.
NPI
Not required.
57.
OTHER PRV ID
Enter the 9-digit Arkansas Medicaid provider ID number
of the billing provider in first line of field.
58. A,
B, C
INSURED’S NAME
Inpatient and Outpatient: Comply with the UB-04
Manual’s instructions when applicable to Medicaid.
59. A,
B, C
P REL
Inpatient and Outpatient: Comply with the UB-04
Manual’s instructions when applicable to Medicaid.
60. A,
B, C
INSURED’S
UNIQUE ID
Inpatient and Outpatient: Enter the patient’s Medicaid
identification number in first line of field.
61. A,
B, C
GROUP NAME
Inpatient and Outpatient: Using the plan name if the
patient is insured by another payer or other payers,
Follow instructions for field 60.
62. A,
B, C
INSURANCE
GROUP NO
Inpatient and Outpatient: When applicable, follow
instructions for fields 60 and 61.
63. A,
B, C
TREATMENT
AUTHORIZATION
CODES
Inpatient: Enter any applicable prior authorization,
benefit extension or MUMP certification control number
on line 63A.
Outpatient: Enter any applicable prior authorization or
benefit extension numbers on line 63A.
64. A,
B, C
DOCUMENT
CONTROL
NUMBER
Field used internally by Arkansas Medicaid. No provider
input.
65. A,
B, C
EMPLOYER NAME
Inpatient and Outpatient: When applicable, based upon
fields 51 through 62, enter the name(s) of the individuals
and entities that provide health care coverage for the
patient (or may be liable).
66.
DX
Diagnosis Version Qualifier. See the UB-04 Manual.
45
Arkansas Medicaid Hospital Billing Tips
Field #
Field name
Description
67.
A-H
(blank)
Inpatient and Outpatient: Enter the ICD-9-CM diagnosis
codes corresponding to additional conditions that coexist
at the time of admission or develop subsequently, and
that have an effect on the treatment received or the
length of stay. Fields are available for up to 8 codes.
68.
(blank)
Unassigned data field.
69.
ADMIT DX
Required for inpatient. See the UB-04 Manual.
70.
PATIENT REASON
DX
See the UB-04 Manual.
71.
PPS CODE
Not required.
72
ECI
See the UB-04 Manual. Required when applicable (for
example, TPL and torts).
73.
(blank)
Unassigned data field.
74.
PRINCIPAL
PROCEDURE
Inpatient: Required on inpatient claims when a
procedure was performed. On all interim claims, enter the
codes for all procedures during the hospital stay.
Outpatient: Not applicable.
74a74e
CODE
Principal procedure code.
DATE
Format: MMDDYY.
OTHER
PROCEDURE
Inpatient: Required on inpatient claims when a
procedure was performed. On all interim claims, enter the
codes for all procedures during the hospital stay.
Outpatient: Not applicable.
CODE
Inpatient claims only. Other procedure code(s).
DATE
Inpatient claims only. Format: MMDDYY.
75.
(blank)
Unassigned data field.
76.
ATTENDING NPI
NPI not required.
QUAL
Enter 0B, indicating state license number. Enter the state
license number in the second part of the field.
LAST
Enter the last name of the primary attending physician.
FIRST
Enter the first name of the primary attending physician.
OPERATING NPI
NPI not required.
QUAL
Enter 0B, indicating state license number. Enter the
operating physician’s state license number in the second
part of the field.
LAST
Enter the last name of the operating physician.
FIRST
Enter the first name of the operating physician.
OTHER NPI
NPI not required.
77.
78.
46
Field #
Field name
Description
QUAL
Enter 0B, indicating state license number. Enter the state
license number in the second part of the field.
LAST
Enter the last name of the primary care physician.
FIRST
Enter the first name of the primary care physician.
79.
OTHER
NPI/QUAL/LAST/FI
RS
Not used.
80.
REMARKS
For provider’s use.
81.
CC
Not used.
47
Arkansas Medicaid Hospital Billing Tips
Requesting Crossover Forms
Print out the request form in section V of your provider manual. Specify that you are requesting
form HP-MFR-001.
Fax or mail your request to:
Fax
(501) 374-0549
Mailing Address
HP Enterprise Services
P.O. Box 8033
Little Rock, Arkansas 72203
48
Tips for Completing Crossover Forms
Pay attention to examples of completed forms.
Use Medicaid Form Request HP-MFR-001.
Follow the instructions for completing Outpatient crossover forms.
Follow the instructions for completing Inpatient crossover forms.
Use the Medicaid 9-digit Provider Number only (No NPI).
Since documents are scanned, ensure you write legibly and stay within the fields.
Use black ink.
49
Arkansas Medicaid Hospital Billing Tips
MEDICAID FORM REQUEST
Provider ID #: _____________________________
Name: _________________________________________
Taxonomy Code:_______________________ ___
Address: _______________________________________
Attn: _________________________________
______________________________________________
City: ____________________________________
State/ZIP: ______________________________________
Please indicate the quantity of forms below:
_____ DCO-645 (Hospital/Physician/Certified Nurse Midwife
Referral for Newborn Infant Medicaid Coverage)
_____ DMS-2609 (Primary Care Physician Selection
and Change Form)
_____ DHS-754 (Hospice/INH Claim Form)
_____ DMS-2615 (Prescription & Prior Authorization
Request for Nutrition Therapy & Supplies)
_____ DMS-26-V (Visual Care)
_____ DMS-2692 (Request for Private Duty Nursing
Services Prior Authorization and Prescription
Initial Request or Recertification)
_____ DMS-601 (Request for Targeted Case Management
Prior Authorization for Beneficiaries Under Age
21)
_____ DMS-0685-14 (Medicaid Prescription Drug
Program Prior Authorization (PA) Request for
Extension of Benefits)
_____ DMS-615 (Sterilization Consent Form)
_____ DMS-2698 (Certification Statement for Abortion)
_____ DMS-618 (Personal Care Assessment and Service
Plan)
_____ HP-AR-004 (Adjustment Request Form Medicaid XIX)
_____ DMS-619 (Consent for Release of Information)
_____ HP-CI-003 (Medicaid Claim Inquiry Form)
_____ DMS-630 (Referral for Medical Assistance)
_____ HP-CR-002 (Explanation of Check Refund)
_____ DMS-632 (DDTCS Transportation Survey)
_____ HP-MFR-001 (Medicaid Form Request)
_____ DMS-633 (Mental Health Services Provider
Qualification form for LCSW, LMFT and LPC)
_____ HP-MC-001 (Inpatient Services MedicareMedicaid Crossover Invoice)
_____ DMS-640 (Occupational, Physical and Speech
Therapy for Medicaid Eligible Beneficiaries
Under Age 21 Prescription/Referral)
_____ HP-MC-002 (Long Term Care Services
Medicare-Medicaid Crossover Invoice)
_____ DMS-671 (Request for Extension of Benefits for
Clinical, Outpatient, Laboratory and X-Ray
Services)
_____ HP-MC-003 (Outpatient Services MedicareMedicaid Crossover Invoice)
_____ DMS-679 (Medical Equipment Request for Prior
Authorization & Prescription)
_____ HP-MC-004 (Professional Services MedicareMedicaid Crossover Invoice)
_____ DMS-694 (EPSDT)
_____ PUB-019 (Sterilization Consent Form Information
for Women)
_____ DMS-699 (Request for Extension of Benefits)
_____ PUB-020 (Sterilization Consent Form Information
for Men)
_____ DMS-2606 (Acknowledgement of Hysterectomy
Information)
Received
Date
By
Mailed
Date
Qty
50
51
Arkansas Medicaid Hospital Billing Tips
Outpatient Crossover
52
53
Arkansas Medicaid Hospital Billing Tips
Inpatient Crossover
54
Common Billing Errors
Refer to the chart below to learn how to correct common billing errors that are associated with
certain Explanation of Benefits (EOB) codes:
EOB Code
Error
Method of Correction
263 and 267
Beneficiary is partially or totally
ineligible for the DOS.
Verify the beneficiary is eligible for all
claim dates of service. Resubmit the
claim/portion of the claim for the time of
eligibility.
282 and 284
Beneficiary has Medicare
coverage.
Bill Medicare first. Submit crossover claim
to Medicaid after Medicare adjudication.
208
Beneficiary aid category 69 is
limited to family planning
services only.
Verify that the original claim has a family
planning diagnosis and procedure code.
Correct and resubmit the claim.
252
Medicaid ID number submitted
does not match patient’s name
on Medicaid ID card.
Verify eligibility through Medicaid’s
electronic eligibility system and resubmit
the claim with correct information.
792 or 900
Ten days post-op care is
included in the payment for the
surgical procedure. Pricing of
this procedure includes services.
A related service has been paid
preventing payment of this code.
Post-op care claims filed after surgery will
deny correctly with EOB 792. No
additional payment is made. An
adjustment must be filed to bill the
surgery if post-op care is paid before the
procedure is billed.
900
venipuncture
Pricing of this procedure
includes related services. A
related service has been paid
preventing payment of this code.
Venipuncture is included in lab work when
performed on the same DOS by the same
provider. An adjustment must be filed to
bill for lab work if venipuncture has been
paid.
469 or 470
Duplicate billing. Claim is
identical to another claim for
DOS, performing provider,
procedure, TOS and price.
Verify that the service is not a duplicate
bill. Resubmit the corrected claim
103
Claim does not meet the timely
filing requirements for Medicaid.
Claims must be received by HP
ENTERPRISE SERVICES within 12
months from the “To” DOS. Claims
received beyond this deadline will not be
paid. Claims for global services (i.e.
claims for prenatal, delivery and
antepartum care) must be received 12
months from the date of delivery.
952
Service requires Primary Care
Physician referral.
Resubmit the claim with the corrected
PCP information required for adjudication.
199
ARKids First-B beneficiary is
older than 18 years old.
ARKids First-B beneficiary’s eligibility
ends on their 19th birthday. The “from”
DOS cannot exceed the 19th birthday.
55
Arkansas Medicaid Hospital Billing Tips
Helpful Tips and Procedures
Benefit limit for adult inpatient stay is 24 days. No extensions.
On the fourth day of an inpatient stay and the patient remains in the hospital, you must
follow the MUMP policy. You should request an extension for the fifth day and thereafter
from AFMC.
Inpatient days for children’s categories are not limited to 24 days. They have unlimited
inpatient days.
Levels of Emergency Claims
Initial Assessment - Evaluate the patient’s complaint or presenting condition to
determine if it is a true emergency.
Includes payment for all tests, such as lab and X-ray, to make the determination.
Emergent - True Emergency services do not require a PA (Prior Authorization) and PCP
referral is not needed.
You must bill using condition code 88.
Non Emergent - Consists of outpatient services that were not deemed a true emergency,
such as:
A.
B.
C.
D.
E.
F.
G.
Treatment and examination
Lab and X-Ray
Observation bed status
Fetal monitoring
Claims count against the benefit limit of 12 outpatient visits
You can request an extension of benefits
PCP referral required
Contact AFMC for an extension of inpatient days.
See section 244.000 of the Hospital provider manual for more information on procedure
codes that require a prior PA.
When billing for sterilizations, you must submit a paper claim. Include a signed DMS615 Sterilization Consent Form. The beneficiary must be 21 on the date the consent was
signed. The sterilization surgery must take place after the required 30-day waiting period
but not more than 180 days after the beneficiary signed the consent form. Exceptions,
such as premature delivery, do apply.
For emergency abdominal surgery, be sure to sign all fields that require a signature.
Hysterectomies require a PA unless they are performed due to malignant neoplasm,
carcinoma in-situ and severe dysplasia. You must submit a paper claim. Include a
DMS-2006 form with your claim.
56
HP Enterprise Services Contact Information
Providers needing assistance on billing, enrollment or technical support should call HP
Enterprise Services at one of the following assistance numbers:
1-800-457-4454 (outside of Little Rock but in-state)
(501) 37612211 (local or out-of-state)
Depending on the type of assistance needed, follow the instructions in the phone system to
reach the appropriate department. The provider assistance departments are:
Provider Assistance Center - The provider assistance center is open weekdays 8 a.m. to
5 p.m. to assist providers with claim issues, billing questions and denials.
EDI support center - The EDI Support Center is open weekdays 8am to 5pm to assist
providers with electronic claim submission issues, 997 batch responses, PES software
downloads and setup support, software training and data transmission failures.
HP Enterprise Services Provider Enrollment - The HP Enterprise Services-Medicaid
Provider Enrollment Unit is open weekdays 8am to 5pm to assist providers with
enrollment in the Arkansas Medicaid program, changing PCP caseloads and updating
demographic information.
HP Enterprise Services Provider Representatives - HP Enterprise Services Provider
Representatives are available to visit your facility by appointment. They assist providers
with billing issues, software delivery and setup, escalated issues and policy questions.
See the Arkansas Medicaid website for a list of representatives by counties.
Research Analyst - The PAC Research Analyst assist providers with escalated billing
issues, claim appeals and special processing requests. See the Arkansas Medicaid
website for contact information by county.
57