New Hire Form – Expanded Version
advertisement

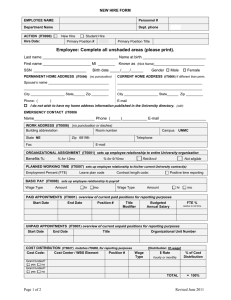
EMPLOYEE NAME Personnel # Department Name Dept. phone New Hire Form Employee: Complete all unshaded areas (please print). ACTIONS From (MM/DD/YYYY) DESCRIPTION OF ACTION New Hire ACTION (IT0000) Primary Position # Student Hire CrHrs Volunteer Hire Primary Position Title Employee Group --Non-resident alien? yes no Federal Employee PERSONAL DATA (IT0002) Last name _________________________________ Name at birth ____________________ First name _________________________________ Middle initial Known as (Nick Name) Birth date ___________________________ ______/______/__________ SSN __________ (no period) _________________________ Male Gender Female ORGANIZATIONAL ASSIGNMENT (IT0001) sets up employee relationship to entire University organization Benefits %: % for 12mo % for 9/10mo CURRENT POSITIONS AT THE UNIVERSITY Position Number Ret/Ancil Position Title Not eligible Staffing Percent This Position 2 3 4 5 6 TOTAL PERMANENT HOME ADDRESS (IT0006) = 100 % (no punctuation or dashes) Spouse’s name (if applicable)________________________________________________________ 1 ______________________________________________________________________________ 2 ______________________________________________________________________________ City _____________________________________ State ______ Zip ____________ - _____ Telephone (________) _______________________ E-mail _____________________________ I do not wish to have my home address information published in the University directory. (xdir) CURRENT HOME ADDRESS (IT0006) (no punctuation or dashes) c/o_____________________________________________________________________________ 1 ______________________________________________________________________________ 2 ______________________________________________________________________________ City _____________________________________ State ______ Zip ____________ - _____ Telephone (________) _______________________ E-mail _____________________________ continued next page Page 1 of 3 Revised June 2011 2 PAF WORK ADDRESS (IT0006) (no punctuation or dashes) Building abbreviation Room number State NE Campus Zip 68198- UNMC Telephone E-mail Fax EMERGENCY CONTACT (IT0006) (no punctuation or dashes) Name___________________________________________________________________________ Telephone (________) _______________________ E-mail _____________________________ PLANNED WORKING TIME (IT0007) sets up employee relationship to his/her current University contract(s) Positive time reporting Employment Percent (FTE) Contract length code: Leave plan code BASIC PAY (IT0008) sets up employee relationship to payroll Wage Type Amount hr mo Wage Type Amount hr mo Wage Type Amount hr mo Wage Type Amount hr mo COST DISTRIBUTION (IT9027) matches IT0008, for reporting purposes Cost Code: Cost Center / WBS Element Position # Wage Type [Distribution: 01-wage] $ Rate % of Cost hourly or monthly Distribution Grant funded? yes no Grant funded? yes no Grant funded? yes no Grant funded? yes no TOTAL = 100% PAID APPOINTMENTS (IT9001) overview of current paid positions for reporting purposes Start Date End Date Position # Title Modifier Budgeted Annual Salary FTE % relative to full time UNPAID APPOINTMENTS (IT9001) overview of current unpaid positions for reporting purposes Start Date End Date BANK DETAILS (IT0009) Title Organizational Unit Number Attach Bank deposit form Change DEPT to HOME TAX AREA (IT0207): NE TAX WITHHOLDING W4 / W5 (IT0210) Attach Form W-4 (required for all new/returning) / Form W-5 (optional) Completed by Payroll RESIDENCE STATUS (I-9) (IT0094) C -Citizen N -Non-citizen Attach Form I-9 with photocopies of documentation (required for all new/returning) A –Non-Resident Alien continued next page Page 2 of 3 Revised June 2011 3 PAF ADDITIONAL PERSONAL DATA (IT0077) Ethnicity (select one) Hispanic/Latino Not Hispanic/Latino Race (select multiple) American Indian/Alaskan Native Asian Black or African American Native Hawaiian or Other Pacific Islander White Unknown Veteran status Discharge Date: _________________ Non Veteran Special Disabled Veteran Vietnam Era Veteran Other Protected Veteran Recently Separated Veteran Armed Forces Service Medal Veteran Disabled Veteran Unknown Military status Not applicable Medicare eligible Yes No Active National Guard Disability Yes No Date disability determined ____/____/________ DATE SPECIFICATIONS (IT0041) (mm/dd/yyyy) I-9 Date required (I9) First Working Day required (40) University Service Date (UD) Leave Accrual Date Health Professions Tracking1 (HP) Health Professions Contract1 (HC) (Begin date of the original health professions contract) (Begin date of the current health professions contract) Graduate Faculty (GR) Other __________________________ 1For (01) new faculty hired on Health Professions Appointments HP and HC are the same date. MONITORING OF TASKS (IT0019) (mm/dd/yyyy) Probation Expires (01) HP Contract Expires (07) Appointment Expires (non HP) (02) Employment Agreement Expires (EA) EDUCATION (IT0022) Enter only highest and most recent. (not required for student workers) Date of graduation ____/____/_____ Institution name (acronym preferred)_____________________________ Certificate/Degree _________________ Is this the highest possible degree in your field? Yes No ---------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------- (additional degrees, if any) Date of graduation ____/____/_____ Institution name (acronym preferred)_____________________________ Certificate/Degree _________________ Is this the highest possible degree in your field? Yes No QUALIFICATIONS (IT0022) ( licenses and certifications, if applicable) License _____________________________________ Certification ___________________________________ Other _______________________________________ Other ________________________________________ EMPLOYEE SIGNATURE ___________________________________________________ date____________________________ ADDITIONAL COMMENTS OR EXCEPTIONS: APPROVAL SIGNATURES: ___________________________________ date____________ ___________________________________ date____________ Attachments Attachments Form W-4 (required for all new/returning employees) / Form W-5 (optional) Form I-9 with photocopies of documentation (required for all new/returning employees) Bank deposit form Correspondence and supportive documentation Page 3 of 3 Revised June 2011