Seminal Semen analysis Analysis
advertisement

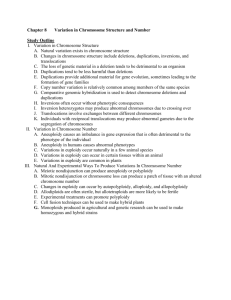
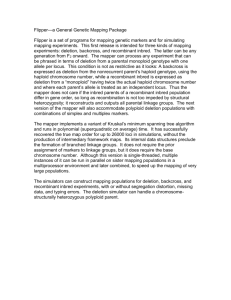
F&S 2829 revised Lardone et al. AZFc subdeletions in infertile Chilean men AZFc partial deletions in Chilean men with severe spermatogenic failure María C. Lardone, B.S.,a Daniela A. Parodi, M.Sc.,a Mauricio Ebensperger, M.D.,b Paulina Peñaloza, M.D.,b Valeria Cornejo, M.D.,b Raúl Valdevenito, M.D.,c Ricardo Pommer, M.D.,a and Andrea Castro, M.Sc.a a Institute of Maternal and Child Research, School of Medicine, University of Chile, Santiago, Chile; bSan Borja Arriarán Clinical Hospital, Santiago, Chile; cJosé Joaquín Aguirre Clinical Hospital, School of Medicine, University of Chile, Santiago, Chile. Received August 17, 2006; revised January 4, 2007; accepted January 5, 2007. This study was supported by grant no. 1030984 from the National Fund for the Scientific and Technological Development (FONDECYT), , Chile,. Reprint requests: Andrea Castro, Institute of Maternal and Child Research, School of Medicine, University of Chile, Santa Rosa 1234, Santiago, Chile (FAX: 56-2-4247240; E-mail: acastro@med.uchile.cl). 0015-0282/07/$32.00 doi:10.1016/j.fertnstert.2007.01.038 Fertility and Sterility® Vol.##, No.##, Month 2007 Copyright ©2007 American Society for Reproductive Medicine, Published by Elsevier Inc. Lardone et al. 1 CAPSULE The analysis of DAZ-SNVs and STS-specific AZFc markers in Chilean men with severe spermatogenic failure, and controls with normal spermatogenesis, showed that AZFc subdeletions are not associated with severe impairment of spermatogenesis. Objective: To determine the prevalence of AZFc subdeletions in infertile Chilean men with severe spermatogenic impairment. Design: Prospective analysis. Setting: University infertility clinic. Patient(s): Ninety-five secretory azo/oligozoospermic men without AZFc Y chromosome microdeletions: 71 whose testicular histology showed severe spermatogenic impairment and 24 who exhibited reduced testicular volume and elevated serum FSH levels. As controls, we studied 77 men (50 fertile and/or normozoospermic, and 27 with azoospermia and normal spermatogenesis). Intervention(s): Peripheral blood was drawn to obtain genomic DNA for polymerase chain reaction (PCR) digestion assays of DAZ-sequence nucleotide variants and for AZFc-STS PCR after a complete testicular characterization (biopsy, hormonal, and physical evaluation). Main Outcome Measure(s): DAZ genes and AZFc subdeletion types. Result(s): In cases we observed two “gr/gr” subdeletions (2.1%), one with absence of DAZ1/DAZ2 (g1/g2 subtype), and the other with absence of DAZ3/DAZ4 (r2/r4 subtype). Additionally, we found a g1/g3 subdeletion in a patient with Sertoli-cell-only syndrome. In Lardone et al. 2 controls, we observed two gr/gr subdeletions with absence of DAZ1/DAZ2 (2.6%) in a fertile/normozoospermic and in an obstructive azoospermic man. Conclusion(s): AZFc subdeletions do not seem to cause severe impairment of spermatogenesis. Moreover, gr/gr-DAZ1/DAZ2 subdeletions do not appear to affect fertility in Chilean men. Key Words: AZFc partial deletion, male infertility, spermatogenic impairment, Y chromosome, DAZ gene. Y chromosome microdeletions constitute an important etiological factor in spermatogenic failure. Several studies indicate a prevalence of 5% to 20% in subjects with azoospermia or severe oligozoospermia (1, 2), and 25% to 55% in patients with severe testiculopathies, such as hypospermatogenesis, maturation arrest (MA), and Sertoli-cell-only syndrome (SOCS) (3, 4). These deletions were described in three nonoverlapping regions in proximal (AZFa), middle (AZFb), and distal (AZFc) Yq11.2 (5, 6). AZFc is the most frequently deleted region, and men with AZFc deletions have a variable testicular phenotype that may be compatible with sperm recovery at testicular sperm extraction (4, 5). The AZFc region encompasses a complex of three palindromes, the largest spanning 3 Mb with 99.97% identity between its arms. The palindromes are constructed from six distinct families of amplicons, and may have resulted from tandem duplication and inversion during primate evolution. The palindromic complex contains 11 families of transcription units, all expressed in testis. In between these transcription units DAZ genes are organized in two cluster groups of genes in orientation 3′5′:: 5′3′ (7, 8). Lardone et al. 3 Deletion of AZFc removes all four copies of the DAZ gene spanning a 3.5-Mb segment bounded by b2 and b4 amplicons, which serve as substrates for homologous recombination producing complete AZFc deletion (8). DNA sequence alignments within AZFc also reveal the possibility for the formation of subdeletions or partial deletions. Detailed analysis of the AZFc region using new molecular nonrepeated STS markers has confirmed the existence of three such subdeletions, namely, gr/gr, b1/b3, and g1/g3 (also known as b2/b3) (9–11). The most prevalent partial deletion, called gr/gr (12), is caused by recombination between amplicons g and r (g1, r1, and/or r2, with their respective homologous amplicons g2, r3, and/or r4). This subdeletion produces the loss of two of the four copies of the DAZ gene (DAZ1/DAZ2 or DAZ3/DAZ4), one of three copies of the BPY2 gene, and one of two copies of the CDY1 gene (CDY1a). Similarly, others are the outcome of b1/b3 and g1/g3, leading to retention of two DAZ gene copies, two or one BPY2 genes, and two or one CDY1 gene copies, respectively. Several investigators have found an association between gr/gr subdeletions and spermatogenic failure (9, 13–16), whereas others have not (17–20). To determine the contribution of these AZFc subdeletions to male infertility, we assessed their prevalence and associated testicular phenotype in a population of infertile men in Chile with severe impairment of spermatogenesis. We used a combined methodological approach that included the detection of the different DAZ gene copies by SNVs analysis (21) and AZFcspecific STSs (12). Our results showed that the prevalence of partial AZFc deletions was not statistically different between cases and controls. MATERIALS AND METHODS Lardone et al. 4 Patients This study was approved by the Institutional Review Board of the School of Medicine at the University of Chile, San Borja Arriarán Clinical Hospital, and José Joaquín Aguirre Hospital, and all subjects gave their informed consent. We studied 95 Chilean infertile patients with impairment of spermatogenesis, who sought consultation for infertility at the Institute of Maternal and Child Research or at the José Joaquín Aguirre Hospital. The study included 77 controls: 19 healthy and fertile donors with unknown seminal parameters, 31 normozoospermic donors with unknown fertility, and 27 obstructive azo/oligozoospermic men with normal spermatogenesis assessed by testicular biopsy. Donors were Chilean men from the same centers, and their fertility status was presumed by the fact that they reported to have fathered one or more children. All participants underwent an evaluation that included complete physical examination, hormonal studies, and karyotype. Testis volume was measured by ultrasonography and/or Prader orquidometer. Serum testosterone was determined using radioinmunoassay (RIA). LH and FSH were measured by immunoradiometric assay (IRMA). Patients with hypogonadotrophic hypogonadism, hypoandrogenism, chronic diseases, or AZFc Y chromosome microdeletions were excluded. The Y chromosome microdeletion standard analysis was performed using a set of 34 STSs including AZFc markers (PRY, sY254, sY221, sY255, sY202, BPY2, sY283, CDY1, and sY158) as previously described (22). Semen Analysis Semen analysis was performed according to normal standard parameters using the World Health Organization (WHO) criteria (23). The diagnosis of azoospermia was based on the absence of Lardone et al. 5 sperm in at least two separate semen analyses and after centrifugation of semen samples (1,000 g, 5 minutes). The selected infertile men were classified as azoospermic or severe oligozoospermic patients (sperm count 5 million/mL). Testicular Biopsy In secretory or obstructive azo/oligozoospermic infertile men, the testicular biopsy was performed for spermatic recuperation by TESE or for diagnosis. Among the controls, some normozoospermic men (n = 10) were also subjected to testicular biopsy during genital surgery, because of testicular cancer (n = 3) or for non-neoplasic reasons (2 hidrocele, 2 epididymal cysts, and 3 varicocele), at the Urology Service of the San Borja Arriarán Hospital, and all had normal testicular histology. Testicular histology assessment included a qualitative and quantitative analysis of germinal epithelium in 25 tubules, and the modified Johnsen score was calculated (24, 25). According to this score, the tissues were classified in SOCS, complete or incomplete (some foci of spermatogenesis); MA, germ cells until spermatogonia, spermatocyte, or spermatid, which may be complete or incomplete (some tubules show germ cells more developed than the maturation detention stage); and hypospermatogenesis (proportional and quantitative reduction of the different types of germ cells). Combined Analysis of AZFc Partial Deletions A two-step approach was employed to identify partial AZFc deletions. First, screening was performed in all patients to discriminate between DAZ1-DAZ4 gene copies (21) using pairs of primers specific to single nucleotide variants (SNVs)—SNV I, SNV II, SNV III, SNV IV, SNV V (sY587) and sY581, and the STS Y-DAZ3 (Table 1)—and combined with the use of the STS marker sY1291 specific to gr/gr subdeletion (12). A negative result was repeated for Lardone et al. 6 confirmation, and a second step with six additional pairs of primers was used for further characterization: sY1258, sY1197, sY1161, sY1191, sY1206, and sY1201 (12). Second,single PCR reactions were performed. The components of PCR were 1 μL aliquot of the genomic DNA (140 g/mL), 1.5 μL of 10 buffer solution, 0.15 μL of 100 mmol/L of each dNTP, 0.7 μL of each primer (10 μmol/L) and 0.2 μL of Taq DNA polymerase (5 U/μL) (MBI Fermentas) in a total volume of 15 μL. PCR was performed according to the following protocol: amplification by 30 cycles at 94°C for 45 seconds, annealing at 55°C (SNV IV), 58°C (SNV I, SNV II, sY581, sY587, and Y-DAZ3), or 63°C (SNV III) for 60 seconds, and 72°C for 60 seconds. The program was preceded by a 3-minute denaturation step at 94ºC and followed by a final extension step at 72°C for 10 minutes. PCR conditions for sY1291, sY1258, sY1197, sY1161, sY1191, sY1206, and sY1201 were similar except that annealing temperature was 57°C and the reaction consisted of 35 cycles. The PCR result was made visible on a 1.5% agarose gel with ethidium bromide. In all PCRs, a female DNA and a water sample (no template) were included as negative controls. DAZ gene copy-specific restriction analysis was performed after digestion of PCR product. Briefly, 7 μL of each PCR product was incubated with 5 U of the respective restriction enzyme at 37 °C (except for Taq I that uses 63 ºC) during 3 hours in a final volume of 10 μL (Table 1). The fragments were visible on a 3% agarose gel with ethidium bromide. Statistical Analysis Differences in hormonal levels and seminal parameters among groups were calculated with the Kruskal-Wallis test. Differences among frequencies were calculated with both the 2 test and the Fisher’s exact test. P<0.05 was considered statistically significant. Lardone et al. 7 RESULTS By Y chromosome microdeletion standard analysis we diagnosed 8% (8/101) cases (secretory azo/oligozoospermic group) with AZF deletions. We analyzed the presence of AZFc subdeletions in 95 patients with no AZFc deletions, including one patient with AZFa and another with AZFb deletions. No AZF deletions were observed in the 77 control males tested. Semen analysis was performed in 95 cases and 58 controls. In the fertile men control group, no semen analysis was available. Sperm counts are shown in Table 2. We observed a higher percentage of azoospermia in patients with SOCS and complete MA. The hormonal analysis revealed that FSH levels in case subgroups of SCOS, and in those without diagnosis by testicular biopsy, were higher compared with complete or incomplete MA, with hypospermatogenesis, and controls (Table 2). Similarly, cases with higher FSH levels had reduced testicular volumes in a higher proportion than other subgroups. DAZ-SNVs Copy Analysis The results of DAZ gene copy analysis in cases and controls are shown in Table 3 and Table 4, respectively. We observed absence of one or two DAZ genes in 14 out of 77 (18%) controls and in 18 out of 95 (19%) cases. DAZ2 deletions (negative result with SNV III and SNV IV) were observed in 9 cases (9.5%) and 5 controls (6.5%). DAZ3 deletions were detected in 1 (1.3%) control patient and in 2 (2.1%) cases. DAZ4 deletion was found in 2 cases (2.1%) and 4 controls (5.2%). No isolated DAZ1 deletion was found in either cases or controls. Simultaneous DAZ2 and DAZ3 deletions were observed in 1 (1.1%) case and 2 (2.6%) controls. DAZ1/DAZ2 cluster deletion was found in 2 (2.6%) controls and 2 (1.1%) cases. DAZ3/DAZ4 cluster deletion was Lardone et al. 8 observed in 2 (1.1%) cases, but not in controls. Significant differences between case and control groups or subgroups were not observed. DAZ-SNVs and AZFc-STS Combined Analysis The amplification of sY1291 in cases and controls did not show any negative result in patients with absence of DAZ2, DAZ3, DAZ4, or DAZ2/DAZ3 by DAZ-SNVs analysis. In contrast, the absence of sY1291 was associated with the loss of DAZ1/DAZ2 cluster. Similarly, the absence of sY1191 was observed only in patients with DAZ3/DAZ4 deletion. Figure 1 shows the result of AZFc subdeletions analysis in cases and controls with the corresponding complete AZFc region structure of the Y chromosome. Overall, we identified 4 gr/gr subdeletions with two different deletion patterns: one with absence of sY1291 and DAZ1/DAZ2 (subtype g1/g2), and the other with absence of sY1291 and DAZ3/DAZ4 (subtype r2/r4). We also found a patient with a g1/g3 deletion. In addition, in a patient with AZFb deletion, we found an AZFc subdeletion with absence of the sY1258, sY1161, sY1197, sY1191, and sY1291 STSs markers and the DAZ1/DAZ2 gene cluster. The STS sY1258 localizes in the distal end of AZFb, whereas the absence of sY1291 suggests that the distal breakpoint localizes in a region within gr1 and Y1. Deletions involving AZFb and part of AZFc have been named “P5/proximal P1” (26). The frequency of partial AZFc deletions among the secretory azo/oligozoospermic group was 4.2%, and 2.6% in the control group (Table 5). The prevalence of partial AZFc deletions was not statistically different between cases and controls, among the different subdeletions, or among case subgroups. Lardone et al. 9 The normozoospermic man (P1012) who presented a gr/gr-DAZ1/DAZ2 subdeletion had fathered two children, each with a different woman. The boy had the same subdeletion. Further investigation showed that his father exhibited the same gr/gr subdeletion and reported a normal fertility history (currently 63 years old with poor seminal parameters). He had reportedly fathered three more children. We studied the patient’s brother and nephews, who also showed the same subdeletion. Investigation of the family of the azoospermic obstructive control (P195) showed that one of his four brothers carried the same gr/gr subdeletion. This subject had fathered two children, but no semen analysis was available. The other brothers had normal fertility, but no semen or DNA samples were available. DISCUSSION Complete deletion of the AZFc region of the Y chromosome includes the loss of the DAZ gene family and is responsible for most cases of spermatogenic impairment in infertile men. Although this deletion has been associated with a variable testicular or seminal phenotype, it might be compatible with the development of sperm, and therefore has a better prognosis than AZFa or AZFb deletions. In this study, we found a high percentage of Y chromosome microdeletions that included the AZFc region. Three of four patients with AZFc deletions had sperm in their ejaculate or in their testicular extraction procedure. Therefore, our results agree with the clinical characteristics of patients with AZFc deletion described in the literature (1–5, 27). The main contribution of our study was determining the prevalence of AZFc partial deletions in Chilean men carefully characterized by testicular histology. In this study we first applied a DAZSNV-specific gene copy and sY1291 (specific gr/gr subdeletion) analysis in 93 secretory azo/oligozoospermic patients with normal karyotypes and without Y chromosome Lardone et al. 10 microdeletions by a standard assay. We subsequently characterized these subdeletions by investigating six additional AZFc-specific STSs (including sY1191, specific for g1/g3 subdeletion) (9–11). In addition, our study included the analysis of AZFc subdeletions in one patient with AZFb (complete MA) and another with an AZFa deletion (SCOS). By DAZ-SNVs analysis we observed a similar percentage of absence of DAZ copy genes in patients with severe impairment of spermatogenesis, and in controls with normal spermatogenesis and/or fertility. When we studied the presence of STS sY1291 or the other AZFc-STS (sY1258, sY1197, sY1161, sY1191, sY1206, sY1201), we found negative amplifications only in DNA from patients who presented absence of DAZ1/DAZ2 or DAZ3/DAZ4 (Fig. 1). Therefore, these patients with DAZ cluster deletions may represent true AZFc subdeletions. This agrees with the mechanism of homologous recombination between amplicons proposed previously where DAZ genes are deleted in doublets (9–11). In the cases of DAZ2, DAZ3, DAZ4, and DAZ2/DAZ3 presumed deletions, we found no associations with absence of any AZFc-STS, indicating that these SNVs negative results in controls and/or cases may represent gene conversion events and not true deletions (21). Moreover, when we compared the prevalence of each of these negative results, we observed similar results in cases and controls, suggesting that our cases and controls represent a similar Chilean subpopulation, which is mainly of Spanish origin (28). According to that, it has been suggested that some DAZ deletion haplotypes might be polymorphic events associated with specific Y chromosome haplogroups (29). In addition, the Y chromosome sequence described and proposed as reference (RPCI-11) belongs to haplogroup R; consequently, the different DAZ haplotypes should be regarded in the context of certain haplogroups. Lardone et al. 11 We usually found consistent results using DAZ-SNVs combined with AZFc-STS analysis in our cases and controls. However, in cases with deletions of DAZ3/DAZ4, predicted by the combined analysis of SNV I, Y-DAZ3, and sY1291 or sY1191, we found an incongruous result with sY587 attributable to the presence of the 196 bp fragment. Moreover, a nonspecific fragment of 196 bp is amplified in female DNA and in DNA from patients with AZFc microdeletion. Therefore, according to our PCR conditions, it should not discriminate the DAZ3/DAZ4 gene cluster. However, sY587 is a good marker for deletion of DAZ1/DAZ2 cluster since it was congruent with the result obtained by SNV II, SNV III/IV, and sY1291. Additionally, the inconsistent results found with SNV III and SNV IV might be related to the variability in DAZ sequences among individuals (polymorphisms in DAZ-SNVs) or gene conversion events (7, 30). In three cases where we did not detect any negative result by DAZ-SNVs analysis, we found a negative result with the pairs of primers specific to sY1291. This result was considered false after a positive amplification of sY1291 with a second DNA sample. A French study (18), which used DAZ-SNVs and AZFc-STS analysis, found one fertile man who failed to amplify sY1291. The investigators do not report that the negative result was confirmed by a second DNA sample, and explained that it may have a low frequency of Y chromosomes (<0.2%) that lack this evolutionary junction fragment. We did not find an association between gr/gr subdeletions and severe spermatogenic failure. Similarly to other studies (18, 19), we found gr/gr subdeletion with loss of DAZ1/DAZ2 in two men with normal spermatogenesis. This subdeletion was also present in the fertile male relatives studied. Nevertheless, many studies found a positive correlation between gr/gr subdeletions and spermatogenic failure (9, 13–16), but others did not (17–20). This disagreement may be explained by different factors. The study of Lynch et al. (14) would not have found an Lardone et al. 12 association between gr/gr subdeletion and infertility if they had studied only secretory azo/oligozoospermic men and had not included infertile men with sperm count of >20 106 sperm/mL. In contrast to other studies (13–15) where most patients were oligozoospermic, the azoospermic subjects in our study represent approximately 70% of cases. In agreement with this, the quantification of DAZ genes by real-time polymerase chain reaction in a population of 90 infertile men and 50 fertile men concluded that partial deletions of the DAZ genes are associated with oligozoospermia but not with azoospermia (31). In that study, the testicular histology of the oligozoospermic men was not evaluated, and hormonal and testicular volume parameters were not documented. Thus, the population studied would not represent true secretory oligozoospermia but rather obstructive oligozoospermia with normal spermatogenesis. Other aspects contributing to the discrepancy in AZFc subdeletions results may be that some investigators (13, 16) did not use a combined approach to define DAZ gene copies. Instead they used sY1291 and sY1191 as the first step for their AZFc-STS analysis; therefore, they were not able to distinguish subtypes of gr/gr partial deletions, DAZ gene copies, and false negatives. Among the gr/gr subdeletions described in the literature, the DAZ3/DAZ4-CDY1a deletion (subtype r2/r4) showed an association with infertility (18). In our study, we found one gr/gr subdeletion of r2/r4 subtype in one man with incomplete MA but none in the controls, suggesting their possible participation in this type of less-severe spermatogenic impairment. However, this result did not reach statistical significance. Another subdeletion called g1/g3 involving DAZ3/DAZ4 is more frequent in individuals of the N haplogroup (common in northern Europe Lardone et al. 13 and Asia) and has been shown to have no spermatogenic impact (11, 27). In this study, we found one patient with g1/g3 subdeletion, but we could not perform Y chromosome haplotyping. The deletion referred as P5/proximal P1 was found in a patient with AZFb deletion previously determined by the absence of sY113 and sY142 at the proximal and distal breakpoints, respectively. Recently, with the availability of nonrepeated STS, it has been described that the AZFb deletion may overlap AZFc by 1.5 Mb (30). Moreover, homologous recombination between direct repeats (P5 in AZFb and P1.2 in AZFc) was proposed as a mechanism to explain the deletions involving AZFb region and AZFc subdeletion (30). Although we were not able to define the proximal AZFb breakpoint at palindrome P5, we speculated the occurrence of a sole deletion event encompassing AZFb and part of the AZFc region. In summary, we investigated the presence of subdeletions in Chilean azo/oligozoospermic men with severe impairment of spermatogenesis. We used a combined approach of DAZ-SNVs and AZFc-STS. We found gr/gr subdeletions with loss of DAZ1/DAZ2 (g1/g2 subtype) in two men with normal spermatogenesis, and in one man with azoospermia and SCOS. Our results suggest that gr/gr-DAZ1/DAZ2 subdeletions are not sufficient to cause severe spermatogenic impairment. In addition, the participation of gr/gr subdeletion, which involves DAZ3/DAZ4 (r2/r4 subtype), may contribute to some spermatogenic defects, such as incomplete MA or lesssevere spermatogenic impairment. Lardone et al. 14 Acknowledgment: We are grateful to Eduardo Gazzo, Flor González, Eduardo Castro, Marcia Madariaga, and Patricia López for their collaboration with some experimental protocols and the contribution on sample semen analysis and karyotype. REFERENCES 1. Vogt PH. Human chromosome deletions in Yq11, AZF candidate genes and male infertility: history and update. Mol Hum Reprod 1998;4:739–44. 2. Krausz C, Bussani-Mastellone C, Granchi S, McElreavey K, Scarselli G, Forti G. Screening for microdeletions of Y chromosome genes in patients undergoing intracytoplasmic sperm injection. Hum Reprod 1999;14:1717–21. 3. Foresta C, Ferlin A, Garolla A, Moro E, Pistorello M, Barbaux S, et al. High frequency of well-defined Y-chromosome deletions in idiopathic Sertoli cell-only syndrome. Hum Reprod 1998;13:302–7. 4. Foresta C. Y chromosome microdeletions and alterations of spermatogenesis. Endocr Rev 2001;22:226–39. 5. Vogt PH, Edelmann A, Kirsch S, Henegariu O, Hirschmann P, Kiesewetter F, et al. Human Y chromosome azoospermia factors (AZF) mapped to different subregions in Yq11. Hum Mol Genet 1996;5:933–43. 6. Ferlin A, Moro E, Garolla A, Foresta C. Human male infertility and Y chromosome deletions: role of the AZF-candidate genes DAZ, RBM and DFFRY. Hum Reprod 1999;14:1710–6. Lardone et al. 15 7. Saxena R, de Vries JW, Repping S, Alagappan RK, Skaletsky H, Brown LG, et al. Four DAZ genes in two clusters found in the AZFc region of the human Y chromosome. Genomics 2000;67:256–67. 8. Kuroda-Kawaguchi T, Skaletsky H, Brown LG, Minx PJ, Cordum HS, Waterston RH, et al. The AZFc region of the Y chromosome features massive palindromes and uniform recurrent deletions in infertile men. Nat Genet 2001;29:279–86. 9. Repping S, Skaletsky H, Brown L, van Daalen SK, Korver CM, Pyntikova T, et al. Polymorphism for a 1.6-Mb deletion of the human Y chromosome persists through balance between recurrent mutation and haploid selection. Nat Genet 2003;35:247–51. 10. Fernandes S, Paracchini S, Meyer LH, Floridia G, HTyler-Smith C, Vogt P. A large AZFc deletion removes DAZ3/DAZ4 and nearby genes from men in Y haplogroup N. Am J Hum Genet 2004;74:180–7. 11. Repping S, van Daalen SK, Korver CM, Brown LG, Marszalek JD, Gianotten J, et al. A family of human Y chromosomes has dispersed throughout northern Eurasia despite a 1.8-Mb deletion in the azoospermia factor c region. Genomics 2004;83:1046–52. 12. Skaletsky H, Kuroda-Kawaguchi T, Minx PJ, Cordum HS, Hillier L, Brown LG, et al. The male-specific region of the human Y chromosome is a mosaic of discrete sequence classes. Nature 2003;423:825–37. 13. de Llanos M, Ballesca J, Gázquez C, Margarit E, Oliva R. High frequency of gr/gr chromosome Y deletions in consecutive oligospermic ICSI candidates. Hum Reprod 2005;20:216–20. Lardone et al. 16 14. Lynch M, Cram D, Reilly A, O'Brien DA, Baker H, Kretser DM, et al. The Y chromosome gr/gr subdeletion is associated with male infertility. Mol Hum Reprod 2005;11:507–12. 15. Ferlin A, Tessari A, Ganz F, Marchina E, Barlati S, Garolla A, et al. Association of partial AZFc region deletions with spermatogenic impairment and male infertility. J Med Genet 2005;42:209–13. 16. Giachini C, Guarducci E, Longepied G, Degl’Innocenti S, Becherini L, Forti G, et al. The gr/gr deletion(s): a new genetic test in male infertility? J Med Genet 2005;42:497–502. 17. Hucklenbroich K, Gromoll J, Heinrich M, Hohoff C, Nieschlag E, Simoni M. Partial deletions in the AZFc region of the Y chromosome occur in men with impaired as well as normal spermatogenesis. Hum Reprod 2004;20:191–7. 18. Machev N, Saut N, Longepied G, Terriou P, Navarro A, Levy N, et al. Sequence family variant loss from the AZFc interval of the human Y chromosome, but not gene copy loss, is strongly associated with male infertility. J Med Genet 2004;41:814–25. 19. Yang Y, Xiao CY, A ZC, Zhang SZ, Li X, Zhang SX. DAZ1/DAZ2 cluster deletion mediated by gr/gr recombination per se may not be sufficient for spermatogenesis impairment: a study of Chinese normozoospermic men. Asian J Androl 2006;8:183–7. 20. Carvalho CM, Zuccherato LW, Bastos-Rodrigues L, Santos FR, Pena SD. No association found between gr/gr deletions and infertility in Brazilian males. Mol Hum Reprod 2006;12:269– 73. Lardone et al. 17 21. Fernandes S, Huellen K, Goncalves J, Dukal H, Zeisler J, Rajpert De Meyts E, et al. High frequency of DAZ1/DAZ2 gene deletions in patients with severe oligozoospermia. Mol Hum Reprod 2002;8:286–98. 22. Castro A, Zambrano N, Kaune H, Madariaga M, Lopez P, Mericq V. YqTER deletion causes arrest of spermatogenesis in early puberty. J Pediatr Endocrinol Metab 2004;17:1675–8. 23. Laboratory manual of the WHO for the examination of human semen and sperm-cervical mucus interaction. Ann Ist Super Sanita 2001;37:I–XII, 1–123. 24. Johnsen SG. Testicular biopsy score count—a method for registration of spermatogenesis in human testes: normal values and results in 335 hypogonadal males. Hormones 1970;1:2–25. 25. Jezek D, Knuth UA, Schulze W. Successful testicular sperm extraction (TESE) in spite of high serum follicle stimulating hormone and azoospermia: correlation between testicular morphology, TESE results, semen analysis and serum hormone values in 103 infertile men. Hum Reprod 1998;13:1230–4. 26. Repping S, Skaletsky H, Lange J, Silber S, van der Veen F, Oates R, et al. Recombination between palindromes P5 and P1 on the human Y chromosome causes massive deletions and spermatogenic failure. Am J Hum Genet 2002;71:906–22. 27. Ferrás C, Fernandes S, Marques CJ, Carvalho F, Alves C, Silva J, et al. AZF and DAZ gene copy-specific deletion analysis in maturation arrest and Sertoli cell-only syndrome. Mol Hum Reprod 2004;10:755–61. Lardone et al. 18 28. Cifuentes L, Morales R, Sepulveda D, Jorquera H, Acuna M. DYS19 and DYS199 loci in a Chilean population of mixed ancestry. Am J Phys Anthropol 2004;125:85–9. 29. Fernandes AT, Fernandes S, Goncalves R, Sa R, Costa P, Rosa A, et al. DAZ gene copies: evidence of Y chromosome evolution. Mol Hum Reprod 2006;12:519–23. 30. de Vries JW, Hoffer MJ, Repping S, Hoovers JM, Leschot NJ, van der Veen F. Reduced copy number of DAZ genes in subfertile and infertile men. Fertil Steril 2002;77:68–75. 31. Writzl K, Zorn B, Peterlin B. Copy number of DAZ genes in infertile men. Fertil Steril 2005;84:1522–5. Lardone et al. 19 FIGURE 1 AZFc structure and results of AZFc-specific STSs and DAZ-specific SNVs analysis. The ampliconic structure of the AZFc region is shown according to Kuroda-Kawaguchi et al. (8). STSs utilized to detect deletions. Red stars 1 to 4: Position of the four DAZ genes. Black boxes: STS present. Lines: STS absent. Gray boxes: STS that normally amplifies by PCR but assumed to be absent in context of deletion pattern. (A) gr/gr subdeletions identified by absence of sY1291. DAZspecific SNVs analysis distinguishes between those with DAZ1/DAZ2 deletion (g1/g2) in patients P136, P195, P1012, and those with DAZ3/DAZ4 deletion (r2/r4) in patient P171. Deletion identified by absence of sY1258, sY1161, sY1191, sY1197, and sY1291 is referred to as P5/proximal P1 (P10). (B) Blue letters: Ampliconic structure of the AZFc region shown after the b2/b3 inversion. g1/g3 subdeletion identified by absence of sY1191. DAZ-specific SNVs analysis shows absence of DAZ3/DAZ4 (P131). FIGURE 2 Pedigree of the normozoospermic subject with gr/gr-DAZ1/DAZ2 deletion. Crossed rectangles: affected patient (gray box) and relatives. OZ: oligozoospermia; NZ: Normozoospermia. Lardone et al. 20