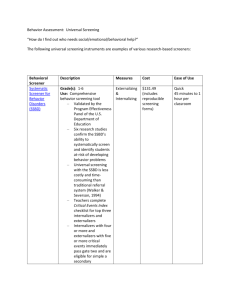
Externalizing Problems in Head Start Children:
advertisement

Externalizing Problems in Head Start Children: An Ecological Exploration Brenda Jones Harden University of Maryland Monique B. Winslow Research Triangle Institute Kimberly T. Kendziora American Institutes for Research Ariana Shahinfar LaSalle University Kenneth H. Rubin University of Maryland Nathan A. Fox University of Maryland Michael J. Crowley University of Maryland Carolyn Zahn-Waxler National Institute of Mental Health Running Head: Externalizing Problems in Head Start Children The authors are grateful for the financial support of the MetLife Foundation in the implementation of this study. We would also like to extend our gratitude to the Head Start children, families, and teachers without whom this research would not have been possible. Externalizing Problems in Head Start Children Externalizing Problems in Head Start Children: An Ecological Exploration ABSTRACT The increased familial and environmental stressors affecting Head Start families over the last two decades have precipitated an escalation of mental health difficulties among participant children (Yoshikawa & Knitzer, 1997). Using an ecological framework (Bronfenbrenner, 1979), this study explored externalizing behavior problems among a group of Head Start children in a suburban county. Children (N=155) were assessed for externalizing behavior problems in the home and classroom. Additionally, parents participated in interviews about a variety of ecological factors related to children’s behavior problems. Almost one-quarter of the children were identified by their parents as having externalizing behavioral problems in the borderline or clinical range. Twice as many girls as boys had borderline or clinical levels of behavioral problems. Child externalizing behavior was positively associated with child internalizing behavior, parent psychological symptomatology, child temperament, family environment, and exposure to community violence. Children with parent-identified externalizing behavior did have specific social problem-solving skills deficits. Additionally, they were observed to have high levels of specific inappropriate behavior, but did not exhibit high levels of teacher-rated behavior problems. The implications of these findings for Head Start program planning are discussed. Externalizing Problems in Head Start Children Externalizing Problems in Head Start Children: An Ecological Exploration Children reared in poverty are experiencing unprecedented challenges to their mental health, including exposure to family and community violence, familial drug involvement, and dwindling community and societal resources. Current evidence points to a strong association between adverse environmental factors, such as poverty, and externalizing (i.e., outer-directed) behavioral problems in children (Sanson, Smart, Prior & Oberklaid, 1993; Bolger, Patterson, Thompson & Kupersmidt, 1995). However, factors within the child (e.g., temperament) and within the proximal ecologies of children (e.g., parent factors) seem to have a greater impact than more distal factors, such as poverty (Shaw, Owens, Vondra, Keenan & Winslow, 1996). Head Start, with its emphasis on serving children living in poverty, is a prime venue for advancing research on the individual and ecological contributions to externalizing problems in young children from low-income backgrounds. Using an ecological framework (Bronfenbrenner, 1977), we examined herein the intra-individual and environmental factors which potentially relate to externalizing behavior problems in Head Start children. Because of the evidence on the primacy of the family ecology, it is a particular focus of this investigation. Externalizing Behavior in Preschool Children Externalizing behavior problems in young children are receiving increasing empirical attention (Campbell, 1995). Research indicates that the most prevalent mental health difficulty in preschool children is externalizing behavior, defined as non-compliance, poor self-control, and problematic social relationships (Campbell, 1990). Empirical interest in preschool behavior problems has also been fueled by evidence of a link between early onset of externalizing behavior problems and antisocial behavior disorders in later childhood and adolescence Externalizing Problems in Head Start Children (Campbell, 1995; Tremblay, Pihl, Vitaro & Dobkin, 1994; Patterson, Reid & Dishion, 1992; Farrington, 1991). Given that externalizing behavior has been identified as a major mental health concern of the preschool years, research which investigates the rate at which this phenomenon occurs in specific populations is important. Campbell (1995) states that approximately 10-15% of preschool children have mild to moderate behavior problems. Data about the prevalence of externalizing behavioral problems in young children from impoverished backgrounds are limited. Although Head Start scholars and practitioners have called for documentation of the prevalence of externalizing behavior among participant children, such data are sparse. There is a growing body of evidence on the prevalence of emotional problems in general in the Head Start population. A national study of Head Start children revealed that 0.5% had emotional or behavioral disabilities based on information received from programs (Piotrkowski, Collins, Knitzer & Robinson, 1994). However, Forness and colleagues (1993) have posited that Head Start children with emotional disturbance remain underidentified at a rate of perhaps 50% of what the rate actually may be. Yoshikawa and Knitzer (1997) have pointed to underestimation of the mental health needs of Head Start children as well, citing the discrepancy between Head Start Program Information Reports (PIR’s) and empirical studies of this phenomenon. These findings suggest that externalizing behavior problems, as one class of mental health difficulty, are underidentified among Head Start children as well. The Ecology of Externalizing Behavior There are multiple risk and protective factors which influence the emergence of externalizing behavior in young children. An ecological framework emphasizes the contribution Externalizing Problems in Head Start Children of the individual and the environment to developmental outcome. Preschool behavioral difficulties have been found to be the result of a complex interplay of intrapersonal and interpersonal factors, including gender (Campbell, 1990), difficult temperament (Sanson et al., 1993), compromised cognitive development (McGee, Partridge, Williams & Silva, 1991), and deficits in social cognition and relationships (Patterson, DeBaryshe & Ramsey, 1989). In terms of gender, a preponderance of evidence exists which indicates that male children, at least in middle childhood and adolescence, are more vulnerable to externalizing behavioral symptoms (Kazdin, 1995). However, the literature is more inconsistent about gender differences during the preschool period (Campbell, 1995). Difficult temperament is predictive of children’s social and behavioral adjustment in preschool and beyond (Rubin, Coplan, Fox & Calkins, 1995; Eisenberg & Fabes, 1992). Recent definitions for difficult temperament in children include emotional lability, poor soothability, distractibility, and hyperactivity (Rothbart & Bates, 1998). Cognitive and social competence are important protective factors which ward against externalizing behavior by giving children psychological resources to manage stressful situations. The resilience literature points to the protective influence of IQ on the development of psychopathology (Masten, Garmezy, Tellegen, Pellegrini & Larsen, 1988). More specifically, cognitive ability has been associated with fewer externalizing behavior problems in studies of young children (e.g., McGee et al., 1991; Lyons-Ruth, Alpern & Repacholi, 1995). Similarly, the capacity to understand social relationships and situations fosters children’s ability to inhibit externalizing behavior (Dodge, 1993). Evidence on one aspect of social cognition - children’s social problem solving - reveals that children who can solve social dilemmas in an appropriate manner have better behavioral adjustment (Dubow, Tisak, Causey, Hryshko & Reid, 1991). Externalizing Problems in Head Start Children Many ecological issues influence the emergence of externalizing behavior in young children. Individual characteristics of parents, such as psychological well-being, have been found to be concurrently and prospectively related to child behavioral problems (Campbell, 1995). A wealth of data exists which points to the relation between maternal depression, quality of parenting, and child outcome (Lyons-Ruth et al., 1993; Zahn-Waxler, Iannotti, Cummings & Denham, 1990). Some studies have documented the tendency of depressed parents to inflate the level of their children’s behavior problems (Fergusson, Lynskey & Horwood, 1993; Webster-Stratton & Hammond, 1988), while other research has suggested that depressed mothers provide veridical appraisals of their children’s problems (Richters, 1992). Family structure and processes have been associated with children’s behavior problems. For example, single parent families are more likely to have children with externalizing behavior problems than families with two parents (Weintraub & Gringlas, 1995). Conflict and disorganization within families result in poor adjustment for children in these environments (Meyers, Taylor, Alvy, Arrington & Richardson, 1992). Discord between marital partners (Webster-Stratton, 1989) and coercive interactions between parents and children (Patterson et al., 1992; Patterson, 1982) are among the factors which have been found to create family climates which breed behavior problems. Children’s experiences in the ecology of the school have a significant impact on their psychological outcomes. Preschool programs, such as Head Start, serve as major socializing agents for young children which can foment or inhibit the emergence of conduct problems in children (Zigler, Taussig & Black,1992). Additionally, young children’s presentation of behavioral difficulties has been found to vary across settings, such as the home, school and clinic Externalizing Problems in Head Start Children (Tynan & Nearing, 1994). This may be partially attributable to the documented disparity between different reporters’ perception of behavior problems (e.g., teacher and parent) (Achenbach, 1987). In the larger ecology, poverty and its concomitants greatly contribute to the development of behavioral difficulties in children. Children from disadvantaged neighborhoods report more stress and as such are prone to exhibit higher rates of aggressive behaviors when compared to their more economically advantaged counterparts (Eamon, 1994). The work of McLoyd (1990) suggests that parental psychopathology is exacerbated by conditions of chronic poverty, which in turn leads to increased psychopathology among children reared in poverty. These less than optimal family environments, engendered by the circumstances of poverty, have been found to be directly related to behavior problems in children (Raadal, Odont, Milgram, Cauce & Mncl, 1994; McLoyd, 1990). Finally, children’s exposure to community violence has an association with emotional problems in young children (Osofsky, 1995). The bulk of this research has focused on psychological outcomes in the internalizing domain, such as Post-Traumatic Stress Disorder (PTSD) as a consequence of community violence exposure. Investigating Behavior Problems in Young Children An abiding theme in the many recent empirical investigations of behavior problems in children is the importance of assessing behavior problems from multi-modal, cross-contextual, and developmental perspectives. Kazdin (1995) argues for a more refined empirical approach, which includes assessing the diverse behaviors that fall within the rubric of conduct problems and using multiple measurement modalities from various significant others. Emphasizing a developmental perspective, Campbell (1995) urges consideration of the potential transient nature Externalizing Problems in Head Start Children of young children’s behavior problems and the environmental factors most likely to affect their functioning (i.e., the family as the primary context for early childhood development). Given that growing numbers of young children are spending time in preschool and child care settings, it has become increasingly important to address their psychological functioning in these contexts as well. With these issues in the foreground, the current study was undertaken to contribute to the literature on the mental health functioning of Head Start children. Specifically, its aim was to inform Head Start program planning relevant to the needs of the growing numbers of participant children with behavior problems. Thus, a major goal of the study was to explore the individual and ecological factors related to behavior problems. Secondly, the study was designed to investigate the problematic behaviors children exhibit in the classroom, from multiple perspectives. A final goal was to examine the social competence of these children, based on scholars’ call for an exploration of this phenomenon in Head Start children (e.g., Raver & Zigler, 1997). Five research questions guided the design of this study. First, what proportion of our sample of Head Start children was reported by parents to have behavior problems? It was anticipated that the rate of behavior problems in our population would exceed the rate reported in normative populations, and would be greater than the proportion which Head Start programs identify in their Program Information Reports. The second question focused on what individual characteristics were associated with externalizing behavior problems in this population of Head Start children. Our hypotheses in this vein were that: 1) a greater number of male than female children would be susceptible to behavioral problems; 2) children with more difficult Externalizing Problems in Head Start Children temperament (i.e. increased emotionality and activity, decreased attention and soothability) would present more externalizing problems; and 3) children with lower cognitive ability (i.e. poorer language skills) would have higher rates of externalizing problems. Third, we sought to identify the ecological factors which were associated with higher levels of externalizing problems. We hypothesized that children with higher levels of behavioral problems would have increased exposure to: 1) parental psychopathology; 2) family conflict; and 3) community violence. A fourth question was whether children’s display of behavior problems at home was reflected in their behavior at school. Our hypothesis relevant to this question was that children who were identified as having high rates of behavioral problems at home (i.e., by their parents) would exhibit high rates of similar behavioral problems at school. Finally, we were interested in the question of how children’s social competence was related to their externalizing behavior. More specifically, we wanted to explore the strategies children with behavior problems used to solve social dilemmas. In addition, we hypothesized that children with more prosocial skills would have lower levels of behavioral problems. In sum, this study was implemented to expand upon the empirical evidence on young children with externalizing disorders by investigating a poor, minority population from a withingroup perspective. Given the call to address mental health issues in Head Start, this research was conducted to contribute to the Head Start literature specifically by examining the multiple ecological factors which are associated with behavior problems in participant children. Additionally, the study was designed to augment available research by employing a multi-modal approach to explore child-specific and environmental factors related to externalizing behavior. Externalizing Problems in Head Start Children Method This study was part of a larger project to design, implement, and evaluate an intervention for Head Start children with behavior problems. The study described herein represents the preintervention component of the project. All children and their caregivers in the target settings were initially interviewed (Phase 1). A subset of children, who were to comprise intervention and comparison groups, participated in a second set of interviews, allowing for a more in-depth analysis of the characteristics of children with behavioral problems (Phase 2). Following is a description of the methods employed to gather these baseline data. Participants. All the children registered to enter ten classrooms of a Head Start program in a suburban county within the greater Washington, DC metropolitan area were initially recruited to participate in the study. These ten classrooms were selected because they were in two public elementary schools serving adjacent communities with similar characteristics. Other Head Start classrooms in this area were dispersed throughout various other schools in dissimilar communities. The schools were also selected because they contained the largest number of Head Start children in the county. A total of 155 children (81% of total population) received parental permission to participate in the first phase of the project. Basically, the children were African-American (99%) and lived in homes with incomes below the poverty line (100%). The average age of the children was 4.1 years (SD=.35). Boys comprised 51% (n=79) of the sample, and girls 49% (n=76). Children (88.4%) were overwhelmingly in the care of their mothers. Caregivers were predominantly single (81.2%), high school graduates (74.2%), and unemployed (69.7%). The average age of the children’s caregivers was 29.9 years (SD=9.1). Further demographic Externalizing Problems in Head Start Children information on the caregivers of these children is found in Table 1. ----------------------------------Insert Table 1 about here ----------------------------------For the second phase of the study, the Child Behavior Checklist (CBCL) was used to identify specific sub-groups of children (see Measures section for a description of the CBCL). A sub-group of children with behavior problems in the clinical or borderline range based on CBCL T scores above 60 (i.e., externalizers) was selected based on parent report (n=42). This subgroup was similar demographically to the larger group of children. Procedures. The data for the current study were collected at two different time points. The first phase of the data collection occurred in the summer before the beginning of the Head Start program year and included the entire sample (N=155). The second phase of data collection occurred in the fall of the Head Start program year and only included a sub-group of the children identified by their parents as having high levels of externalizing behavior. Following are the procedures for each of the phases. Phase 1. Initial assessment of the children and families was conducted in the homes of study participants. Two interviewers completed each visit. While one researcher interviewed the child, the other interviewed the parent. Every measure was read to the children and to the adults to control for differential reading abilities. The home visits lasted about 90 minutes. Each parent was paid $20 for study participation and each child was given a developmentally-appropriate gift. Phase 2. The second data collection phase was completed in the school. Teachers completed their questionnaires independently and were given a monetary contribution to their Externalizing Problems in Head Start Children classroom as an incentive. Children were individually interviewed at school using a hypothetical-reflective social problem solving test in the second month of the academic year. Each child was taken from the classroom to a private room by a trained interviewer. Behavioral observations occurred in the classroom during this same time period. Observations were conducted by trained observers in the classroom in five 1-minute intervals during unstructured and structured activities interspersed throughout the Head Start day on three different occasions (total of 15 minutes per child). Measures and Assessment Protocols. A combination of parent-report, teacher-report, independent observation, and child assessment was used for this study. The initial assessment of the child included a cognitive evaluation and parent-report questionnaires on child behavior problems, temperament, and exposure to violence. The parent assessment included self-report questionnaires regarding parental psychopathology, family functioning, and social support. In the second phase of the study, classroom behavior problems, social competence, and social skills were assessed, as well as the parenting capacity of the caregivers of the children. Parent Questionnaires: Child Behavior. The Child Behavior Checklist (CBCL/4-18; Achenbach, 1991) was used to assess children’s behavioral problems. This is a well established parent-report measure which can be used with children from ages 4 through 18 years. It has been used with normative and clinical samples, including children from minority and low-income backgrounds. Parents state whether 112 behavioral problems apply to their children, using a 3-item response set (i.e., “not true”, “sometimes or somewhat true”, and “very or often true”). Summary scores are derived for the Internalizing behavioral domain (comprised of somatic, anxious-depressed, and withdrawn Externalizing Problems in Head Start Children subscales) and Externalizing behavioral domain (comprised of aggressive and delinquent subscales). Sample items from the aggressive subscale are: “cruelty, bullying, or meanness to others” and “destroys his/her own things”. Sample items from the delinquent subscale are: “doesn’t seem to feel guilty after misbehaving” and “steals at home”. Clinical and borderline cut-off scores have been derived for this measure, based on research with clinical and normative samples. Raw scores are converted into T scores; a T score of 60-63 is in the borderline range, and 64 or over is in the clinical range. Test-retest reliability ranges from 0.87 to 0.95. Child Temperament. The Colorado Child Temperament Inventory (CCTI; Rowe & Plomin, 1977) is a parent-report instrument used to identify temperament types for young children. It is a 30-item questionnaire which yields the following subscales: emotionality; activity; attention; soothability; shyness; and sociability. Rubin and colleagues (1995) have created an emotion dysregulation variable using this measure by subtracting soothability from emotionality, which will be used in this study. Internal reliability data garnered from this study are as follows: emotionality - 0.67; activity - 0.44; attention - 0.28; soothability - 0.46; shyness 0.60; and sociability - 0.55. Parental Psychopathology. The Brief Symptom Inventory (BSI; Derogatis & Spencer, 1982) was used to assess the mental health status of each parent. It is a 53-item self-report questionnaire, which requires respondents to rate each symptom on a 5-point scale of distress (from not at all to extremely) during the last week. There are nine primary symptom dimensions for this scale, but only two of these were selected for this study based on their documented association with child externalizing behaviors. These two subscales and their corresponding internal reliability estimates from this study (presented first in parentheses) and from Boulet & Externalizing Problems in Head Start Children Boss (1991) are: 1) depression (0.86; 0.89); and 2) hostility (0.60; 0.78). The total symptom score (i.e., global severity index) was also ascertained for this study, which had an alpha of 0.95. Family Environment. The Family Environment Scale (FES; Moos & Moos, 1993) was administered to measure the degree of commitment, openness, and disagreement among family members. The short form of this self-report instrument, which contains 54 items, was used in this study. Respondents state whether each statement is true or false for their family. Following are the 6 subscales which comprise this measure with their corresponding alpha coefficients based on data from the current study: conflict (0.63); cohesion (0.62); control (0.27); expressiveness (0.43); organization (0.55); and religiosity (0.54). The overall alpha coefficient for this version has been reported to be 0.65 (Green & Plank, 1994). It is a widely used instrument which, although initially developed with a middle income sample, has been found to be valid with higher risk populations (Moos & Moos, 1993). Child Exposure to Violence. The Violence Exposure Scale for Children - preschool version (VEX-P; Fox & Leavittt, 1995) was used to determine the level of violence to which each child was exposed. Parents were asked to state whether their child had witnessed or experienced 22 different types of violent events occurring at school, at home, and in the neighborhood. This measure was designed for use with this population. Cronbach’s alpha was 0.72 for mild exposure items. Because there was so little variability for severe violence, alpha’s could not be determined in this domain (Shahinfar, Fox, Leavitt & Richters, in press). Family Background. A family information form was devised for this project to obtain data on the families’ socioeconomic status, race/ethnicity, household composition, time child spends with each parent, housing status, religion, and other background issues. Externalizing Problems in Head Start Children Child Assessments: Behavior Problems. Because this was the central variable of interest in this study, three strategies for obtaining these data were employed. First, the parents of the children were interviewed regarding the existence of various behavior problems (see parent questionnaires). Teachers rated the children on the presentation of a variety of behaviors. Finally, independent observers recorded the frequency of children’s display of specific behaviors. Teachers rated the classroom based behavior of the children identified by parents as having high levels of externalizing problems, using the Preschool Behavior Questionnaire (Behar & Stringfield, 1974). This 30-item measure contains 3 subscales: Hostile-Aggressive; Hyperactive-Distractible; and Anxious-Fearful. The responses for this measure are: 1) does not apply; 2) sometimes applies; and 3) frequently applies. The reported reliability for the overall measures is 0.84, and subscale alphas are 0.81 (Hostile-Aggressive), 0.67 (HyperactiveDistractible), and 0.71 (Anxious-Fearful) (Behar, 1977). The children with identified externalizing behavior problems were assessed by trained observers. Training included practice coding of children’s behavior via observing videotapes and children in classrooms. Researchers observed children during five one-minute intervals on three different program days, during structured and unstructured activities (total of 15 minutes). The frequency of children’s appropriate and inappropriate behavior was coded by objective observers. The appropriate category included competent responses to environmental demands. These events were also classified into one of the following categories: solitary play; group play; dramatic play; rough-and-tumble play; and on-task behavior. The inappropriate category included incompetent responses to environmental demands such as withdrawn behavior, negative Externalizing Problems in Head Start Children affect (i.e., sadness and anxiety), hyperactive-inattentive-impulsive behavior, aggressive-reactive and aggressive-initiating behavior. For reliability purposes, a second researcher observed 29% of the observations. Cohen’s kappas averaged 0.93 across all behaviors (SD=0.04; range 0.88-0.97) and 0.92 for the appropriate/inappropriate distinction (SD=0.05; range 0.83-0.98). Social Competence. Two types of data were collected which pertained to this variable. Teachers responded to ten items adapted from the social competence subscale of the Preschool Socioaffective Profile (LaFreniere, Dumas, Capuano, & Dubeau, 1992) for children in the high and low externalizing sub-groups. Socially competent behaviors delineated included cooperating with others, comforts or assists others, and takes pleasure in own accomplishments. Teachers stated whether each behavior “does not apply”, “sometimes applies” or “frequently applies” to a specific child. Scores for responses ranged from 0-2, with a total possible score for this subscale of 20. Internal reliability for this subscale ranged from 0.79 to 0.91. In addition, the Social Problem Solving Test - Revised (SPST-R; Rubin, 1988; Rubin & Rose-Krasnor, 1986) was administered only to the sub-group of children with high rates of parent-identified externalizing behavior problems. The SPST-R is an interview in which children are asked to respond to eight stories, which are accompanied by pictures drawn on 8" by 10" cards, depicting hypothetical social situations. Specifically, they are asked what the central character would do or say to resolve the given social problem, involving either object acquisition or friendship initiation. Children are also asked what they would do if faced with the same situation. Each response was coded for its category membership (i.e. prosocial, agonistic, trade/bribe, inappropriate, authority intervention, and manipulate affect) and for its flexibility (response differed in category from other responses). Incompetent social problem solving skills Externalizing Problems in Head Start Children were determined by the combined score for agonistic and inappropriate strategies. Competent social problem solving skills were defined as the use of prosocial strategies and the receipt of a high score (>2) on flexibility. One third of the children’s responses were coded by two researchers, which yielded a kappa of 0.88. Cognition. The Peabody Picture Vocabulary Test - Revised (PPVT-R; Dunn & Dunn, 1981) was administered to each child in the first phase of the study. The PPVT-R is a widely used test of receptive vocabulary which is highly correlated with child cognitive functioning. Children are shown a group of four pictures and are asked to point to the picture which corresponds to the word given by the examiner. The measure can be used from the preschool period to adulthood. A standard score is derived from the measure which is based on a large, nationally representative sample. Results Following are the results from the two phases of the project. The first phase of the project included all 155 children and parents in the study. Analysis of data collected during this phase addresses the proportion of children with externalizing problems and the relations between child externalizing behavior and child-specific and ecological factors. The second phase of the project focused on a sub-group of children, with high rates of parent-identified behavioral problems (n=42). Data analyses in this phase explores the social competence and classroom behavior of the sub-group of children and the relations between these variables. Descriptive data on the full sample and the externalizing sub-group are presented in Table 2. ----------------------------------Insert Table 2 about here Externalizing Problems in Head Start Children ----------------------------------Phase 1. Prevalence and correlates of externalizing behavior in Head Start children Based on the T scores of the parent-report of the CBCL, 23.7% of the children assessed had externalizing behavior problems in the clinical (15.8%) or borderline (7.9%) range. An examination of the externalizing subscales of the CBCL revealed that 9.7% of the children were reported to have aggressive behavior and 11.0% delinquent behavior in the clinical or borderline ranges. Further, 6.5% of the children were identified as having internalizing difficulties in the clinical or borderline range. Although there was no difference between the average CBCL externalizing behavior Tscores of boys and girls in this study, twice as many girls exhibited externalizing behavioral problems as boys. Fifteen percent of boys and 32% of girls were reported by their parents to have externalizing behavior problems in the clinical or borderline range. Chi square analysis revealed a significant difference between the proportions of boys and girls with externalizing behavior (X2(1)=5.8, p<.02) . This pattern persisted with specific types of externalizing behavior. In regard to aggressive behavior, 14.4% of the girls but only 5.1% of the boys reached the borderline or clinical range. Similarly, 14.4% of the girls were reported to have delinquent behavior and 7.6% of the boys were. Graphic depictions of the proportion of girls and boys who have borderline or clinical externalizing behavior problems are presented in Figures 1 and 2. ---------------------------------------Insert Figures 1&2 about here Externalizing Problems in Head Start Children ---------------------------------------As portrayed in Table 3, externalizing behavior problems in children were significantly associated with several child-specific variables. Externalizing problems were positively related to internalizing symptoms, r(154)=.53, p<.001, and negative emotionality (temperament), r(154)=.55, p<.001. Significant negative associations were found between externalizing behavior and the temperament variables of attention, r(154)=-.23, p<.01, and soothability, r(154)=-.17, p<.05. Externalizing behavior was significantly related to emotion dysregulation (i.e., temperament variables of emotionality minus soothability), r(154)=.49, p<.001. Nonsignificant relations emerged between externalizing behavior and PPVT scores. ----------------------------------Insert Table 3 about here ----------------------------------Several ecological variables had significant associations with externalizing behavior in children. Every symptom of parental psychopathology assessed was strongly associated with child externalizing problems (for total BSI: r(154)=.42, p<.001). Although caregiver marital status was not correlated with child externalizing problems (the majority of the sample was single), the amount of time children spent with their biological mothers, fathers, or other caregivers was. Higher rates of externalizing problems were associated with less time spent with the child’s father, r(154)=.25, p<.01. Chi square analysis comparing children who were with their fathers more than half the time and less than half the time revealed a significant difference between the numbers of children with externalizing behavior in each group (X2 (1)=5.2; p=.02. Children who spent less than half the time with their fathers were more likely to have Externalizing Problems in Head Start Children externalizing behavioral problems. Family environment was also highly correlated with child externalizing problems. Child behavior problems were positively related to family conflict, r(154)=.30, p<.01, and negatively associated with family organization, r(154)=-.21, p<.01. Regarding larger ecological variables, exposure to community violence was positively related to externalizing problems, r(154)=.25, p<.01. Because of the gender findings in this study, correlations were conducted separately for boys and girls; similar patterns of association were found for both groups. The correlations between externalizing behavior and the ecological variables for the total sample are presented in Table 4. ----------------------------------Insert Table 4 about here ----------------------------------Phase 2. Classroom behavior and social competence in Head Start children with high rates of parent-identified externalizing behavior Classroom behavior was assessed for the sub-group of children who were identified with high levels of externalizing behavior problems. Teachers reported an average of 13 out of 30 possible classroom behavior problems overall. Following are the average levels of behavior problems reported by teachers in each of the three categories: Anxious-Fearful M=2.6 (SD=3.1); Hostile-Aggressive M=3.5 (SD=4.8); and Hyperactive-Distractible M=2.6 (SD=2.6). The mean for teacher-rated social competence was 9.9 (SD=5.0) out of a possible total score of 20. Descriptive data on behaviors in the classroom as observed by independent raters are summarized in Table 5. Provided is the proportion of the 15-minute observation period in which Externalizing Problems in Head Start Children children were engaged in specific behaviors. Children with externalizing problems spent the majority of the observed time displaying appropriate behavior. Most of the appropriate observed behavior were when children were involved in on-task activities during structured and unstructured times (e.g., attention at circle time, compliance with teacher, focused exploratory play). They played in groups more than they did in a solitary manner. The majority of their inappropriate behavior consisted of hyperactive-impulsive behaviors. These children did not tend to exhibit aggressive behavior nor display negative affect. ----------------------------------Insert Table 5 about here ----------------------------------The relation between teacher-rated social competence and specific child variables was explored. There was a significant relation between teacher ratings of social competence and teacher ratings of three types of behavior problems: Hostile-Aggressive, r(40)= -.46, p<.01; Anxious-Fearful, r(40)= -.44, p<.01; and Hyperactive-Distractible, r(40)= -.58, p<.001. In contrast, a non-significant relation was found between teacher-rated social competence and social problem-solving skills. The relation between teacher-rated behavioral problems and the types of solution to hypothetical social dilemmas which children selected was also explored for the group of children with high levels of parent-identified externalizing behavior. Children rated as hostile-aggressive by their teachers had less relevant social problem solving strategies, r(40)= -.34, p<.05. The more anxious-fearful children were, the less likely they were to use relevant solutions, r (40) = -.37, p<.05, flexible solutions, r(40)= -.39, p<.05, and prosocial solutions, r(40)=-.56, p<.01 to Externalizing Problems in Head Start Children solve social dilemmas. Children identified by teachers as having hyperactive-distractible behaviors were less likely to provide prosocial solutions, r(40)= -.39, p<.05. The correlations between teacher-rated behavior problems and social problem-solving skills are summarized in Table 6. ----------------------------------Insert Table 6 about here ----------------------------------Further examination of the social problem solving skills of children with high levels of externalizing problems revealed that they generated prosocial solutions to social dilemmas but also relied on more problematic strategies. Following are the mean proportions of specific strategies children utilized in their solutions to social dilemmas: prosocial strategies - 49% (SD=0.23); authority intervention strategies - 8% (SD=0.14); agonistic strategies (e.g. hitting, biting) - 19% (SD=0.23); manipulate affect strategies - 3% (SD=0.07); trade/bribe strategies - 1% (SD=0.03); and inappropriate strategies - 21% (SD=0.27). Discussion There is a solid evidentiary base for the high rates of externalizing behavior problems among children in poverty (Bolger et al., 1995). Consistent with this literature, the present study documented that almost one quarter of Head Start children present with externalizing behavior problems in a sample of children from low-income, minority backgrounds. In this Head Start sample, a higher proportion of children was identified by their parents as having externalizing behavior problems than in normative samples and in other Head Start samples (Sinclair, Del Homme & Gonzalez, 1993; Lopez, Tarullo, Forness, & Boyce, 2000). However, the children in Externalizing Problems in Head Start Children such studies were identified by their teachers as having behavior problems, not by their parents as occurred in the present study. In a study that included parent reports and observational data, Webster-Stratton and Hammond (1998) documented rates similar to those found in the current study. Kazdin (1995) has suggested that parent and teacher reports are distinct in perspective but equally important for understanding child behavior problems. Parent-reports, in particular, have been found to correlate with clinical judgments about externalizing problems. Individual-Level Contributions: Gender, Temperament, and Cognition The disparity between the proportion of boys and girls with externalizing behavior was unanticipated. Reviews of the literature on gender differences and externalizing behavior during the preschool period reveal inconsistent results (Campbell, 1995). A preponderance of evidence suggests that boys are generally more likely to have externalizing behavioral problems during childhood and adolescence. However, recent evidence indicates that externalizing behavior is increasing among adolescent female populations (i.e., increase in arrest rates overall, and for violent crimes and thefts, etc.) (Office of Juvenile Justice and Delinquency Prevention, 1998). Typically, externalizing females have been understudied despite the data that when compared to non-externalizing females, they are more likely to be psychiatrically impaired, adolescent mothers, single parents, less competent mothers, and mothers of children who become externalizers themselves (Tremblay, 1991). However, empirical attention to externalizing females is increasing. For example, Keenan and Shaw (1997) have reviewed several major studies which address young girls’ behavior problems, underscoring the different presentation and trajectory of psychopathology found among females. One of the issues considered in this review is that language serves as a protective factor for girls who are vulnerable to behavioral Externalizing Problems in Head Start Children problems. The girls in the current study had similarly impoverished language as the boys, which may partially explain their high rates of behavior problems. The higher rates of externalizing behavior problems in girls found in this study may be also attributable to the demographic composition of the sample. For example, AfricanAmerican parents have been found to have higher expectations for their female children than their male children. This is particularly salient among single, low-income mothers who expect their female children to have more responsibility and maturity than their male counterparts (Randolph, Koblinsky, Beemer, Roberts, & Letiecq, 2000; Randolph, 1995). It may also be that boys and girls show the same levels of externalizing problems, but that mothers may view this behavior as more normative in boys than in girls. Further, there is some evidence that adolescent females from low-income families may have poorer outcomes than their male counterparts due to their heightened reaction to family stress and interpersonal conflict (Luthar, 1999). As expected, other child-specific characteristics were also associated with externalizing behavior. Certain temperamental factors may render children more vulnerable to psychological difficulties (Sarason et al., 1993). In the current study, the temperamental variables of negative emotionality, attentional problems, and poor soothability were associated with behavior problems reported by parents. This is consistent with a growing body of research which suggests that children who are hypersensitive and easily emotionally aroused are more likely to demonstrate problems of an externalizing nature (Rubin et al., 1995). The relations between externalizing behaviors and attentional difficulties and internalizing behavior were also anticipated. There is substantial evidence on children with Attention Deficit Hyperactivity Disorder which supports the connection between distractibility Externalizing Problems in Head Start Children and behavior problems (Kazdin, 1995; Barkley, 1990). The relation between externalizing and internalizing behaviors has been increasingly documented among low-income children. There is substantial evidence pointing to the comorbidity between externalizing and internalizing difficulties (see Zahn-Waxler, Klimes-Dougan & Slattery, in press; Zoccolillo, 1992). Although the correlations in this study are partially attributable to response bias (i.e. same respondent is reporting on temperament and both types of behavioral problems), they corroborate findings that have been widely reported in the literature. In contrast, cognitive competence (i.e. PPVT score) did not serve as a protective factor for these Head Start children. This finding is inconsistent with the evidence that cognitive and language ability in children are associated with better psychological adjustment (Olson et al., 1990; Masten et al., 1988; Beitchman, Wilson, Brownlie, Walters, Inglis & Lance, 1996). Perhaps in this sample, because cognition/language was universally low (i.e. mean PPVT score of 62.7 for this sample, which is in the deficit range), it did not have the same buffering effect which it does in normative populations. Additionally, because many of these children had not experienced formal education, their scores on the PPVT may not have been an adequate representation of their cognitive competence, but may have been a reflection of understimulation in their environments. Ecological Influences: The Role of the Family and Community The current investigation corroborated findings of the influence of specific aspects of the family ecology on child outcome in this sample of Head Start children. As expected, parental psychopathology was strongly correlated with child adjustment and behavior. Such findings must be considered seriously in the face of evidence pointing to the exacerbation of the effects of Externalizing Problems in Head Start Children poverty by parental psychopathology (McLoyd, 1998). There is a large corpus of literature which documents the deleterious effects of maternal depression on child outcome, including social and academic difficulties at school, and internalizing and externalizing behavior problems (see Downey & Coyne, 1990 for a review). Recent research has underscored the synergistic impact of maternal depression and poverty on child outcome (McLoyd, 1990; 1998). Another symptom of parental psychopathology explored was hostility. The association between the maternal symptom of hostility and externalizing behavior highlights the negative impact of parental negative emotionality on child adjustment, particularly when poverty is a salient factor (Ackerman, Izard, Schoff, Youngstrom & Kogos, 1999). Similarly, family conflict and disorganization can be particularly damaging for poor, minority children who need structure and stability to counter the effects of poverty on their psychological well-being. One important family factor is underscored by the finding that children who spend less time with their fathers have more externalizing problems. The role of the father, whether living in the home or not, in diminishing behavioral problems in young children has been documented in studies of parenting processes as well as intervention efficacy (Black, Dubowtiz & Starr, 1999; Crockett, Eggebeen, & Hawkins, 1993; Webster-Stratton, 1989). That exposure to community violence is related to externalizing problems in preschool children is also a fairly far-reaching finding. Young children may have an early-onset trajectory toward conduct disorder not only because of the family influences which have been documented in many studies (e.g., Walker et al., 1998), but also due to the impact of factors within the larger ecology such as community violence. Additional findings from this study in relation to violence Externalizing Problems in Head Start Children exposure are described elsewhere (Shahinfar, Fox, Leavitt, and Richters, in press). Other investigations of the effects of violence exposure suggest that parents can buffer the effects of community violence on child psychological adjustment as well (Richters & Martinez, 1993). Behavior Problems in the Context of the Classroom The classroom-focused examination of children with high levels of externalizing difficulties yielded a mixture of anticipated and unanticipated findings. Overall, the data confirmed the disparity found in previous studies between teachers and parents on their perceptions of children’s behavior (e.g., Achenbach et al., 1987). Some studies indicate that teachers are more likely to identify behavior problems in children than parents (Zimmerman et al., 1995), whereas others report they are less likely to do so (Webster-Stratton & Hammond, 1998). In this study of Head Start children, parents identified a large group of children with externalizing problems, and teachers did not concur with their perceptions. One potential reason for this lack of congruence emanates from the evidence that mothers who are depressed perceive their children as more problematic (Field, 1995). The difference in parent and teacher instrumentation is also an issue. The CBCL delineates a much wider range of behaviors than the PBQ does. Additionally, Kazdin (1995) suggests that teachers are basing their assessments on peer interactions and other factors distinct from those which parents consider in their evaluations of child behavior. Finally, teachers in this Head Start system may experience fewer behavioral challenges in their classroom due to the provision of the structure that children need to facilitate the regulation of impulses and affect. Thus, it may be that the behavioral problems of these children are more controlled in the classroom. Clearly the school environment is a necessary Externalizing Problems in Head Start Children venue for intervention with children who have behavioral problems, but it may not be sufficient. Addressing the behavioral issues that arise in the home setting may be just as crucial for children’s optimal development. Independent observers discerned varying levels of specific behaviors in externalizing children. These children were observed to be primarily appropriate in their behavior, a finding which was counter to what was expected. What parents observed in the home was not congruent with what was seen at school by teachers and independent observers, specifically in terms of aggressive behavior. Again, the context of the Head Start environment may have provided children with the structure, rules, and adult support which assisted them to refrain from aggressive acts. Nevertheless, the children’s display of hyperactive and impulsive behavior suggests that their capacity to self-regulate is still compromised. Early difficulties with selfregulation and control may portend later aggressive behavioral difficulties and other socially incompetent behaviors(Campbell, 1995; Eisenberg & Fabes, 1992). Social Competence and Externalizing Behavior There was great variability in the level of social problem-solving skills that these children displayed. Studies of normative populations report variability as well, but also report less generation of incompetent problem-solving strategies (Rubin et al., 1991). Previous research has also pointed to the higher levels of incompetent social problem solving strategies used by aggressive children (Rubin et al., 1991). Because the children whose social problem solving ability was evaluated in this study were in the externalizing group, their incompetence in solving social dilemmas was not surprising. Similarly, the inverse relation found between competent social problem-solving and teacher-rated behavioral problems was expected. Externalizing Problems in Head Start Children In contrast, significant relations were not found between social problem solving and teacher rated social competence. As has been found in studies of social problem solving interventions, children’s ability to solve hypothetical dilemmas does not necessarily translate into behavioral competence in social situations (Shure & Spivak, 1980). Additionally, with the advent of more sophisticated perspective-taking, preschool children are capable of fairly complex prosocial behavior such as sharing, helping, and offering comfort (Eisenberg & Fabes, 1998). The children in the current study demonstrated these qualities overall, but tended to have more difficulty with the arguably more emotionally demanding tasks of negotiating social conflicts and regulating negative behaviors. Methodological Issues Although this investigation has provided insight into the home and school factors related to externalizing problems in Head Start children, there are limitations to this study which should be acknowledged. First, the prevalence data offered by this study should be viewed with caution. This was not an epidemiological study which was population based; the two Head Start centers were not selected based on their representativeness. In addition, behavioral observations and teacher reports were not obtained on the entire population of children (i.e. 155). Thus, some modicum of response bias exists for the first part of the study, since the primary respondent was the child’s parent. In the second phase of the study, the sub-sample was small, which has implications for the adequacy of statistical power to conduct specific analyses. Behavioral observations at baseline were also limited. Additionally, a measure of parenting capacity was not included in the current study. Thus, it was not possible to address the mediating role of parenting skill, style, and interaction with the child on the effect of environmental factors on child Externalizing Problems in Head Start Children outcomes. Finally, the influence of the classroom (e.g. teacher-child relationships, structure) on the display of externalizing behaviors was not examined. Future research should incorporate such a comprehensive, multi-modal approach into an investigation of a group of Head Start children representing entire Head Start systems and classrooms. A more in-depth examination of children’s behavioral problems in the home would be beneficial for understanding the high numbers of behavioral problems identified by parents, as well as for informing program development efforts which incorporate parents and children. Moreover, an exploration of the unique needs and capacities of female children with behavioral problems seems warranted. Observational data could be expanded to include teacher-child and parent-child interactions which could be videotaped for later coding. Finally, a comparison of children receiving and not receiving Head Start services would provide valuable information about the contribution of the school environment to behavioral problems in young children. Implications for Educational and Mental Health Intervention There are multiple practice implications of this study. First, as advocated by Yoshikawa and Knitzer (1997), Head start programs need to place more resources into meeting the mental health needs of their populations. Given that one quarter of children in this study exhibited externalizing behavior problems, interventions should be integrated into Head Start program designs which specifically address this issue. This would be a boon to Head Start teachers, who too often cite having to use precious classroom time for behavior management. Teachers need additional preparation to assist them to understand the needs of these children, as well as to increase their repertoire of effective responses to these behaviors in the classroom. Mental health strategies should be designed to meet the needs of both genders. Although research and Externalizing Problems in Head Start Children intervention often target boys, the findings of this study point to the import of incorporating girls into programmatic initiatives and of addressing their unique needs. Prevention programs on all levels (Simeonsson, 1991) should be established with a goal of assisting all Head Start children to behave optimally in the classroom. Models such as the FAST Track program (Bierman, Coie, Dodge, Greenberg & McMahon, in press) and First Steps to Success (Walker et al., 1998) are examples of school-based comprehensive interventions for young children which have resulted in improved child and family outcomes. Such models can be easily adapted for Head Start populations. This comprehensive, program-driven approach would be more appropriate than the current practice in many Head Start programs to “parachute in” part-time consultants to address the mental health needs of children. Child-targeted interventions can be designed to address the emotional, social, and behavioral needs of all Head Start children (see Forness, Serna, Kavale & Nielsen, 1998; Walker, Colvin & Ramsey, 1995; Greenberg, Kusche, Cook & Quamma, 1995; Shure & Spivak, 1980). Programs with the goal of promoting the social competence of young children, in areas such as social problem solving skill and prosocial peer relationships can be adapted for Head Start populations. Similarly, strategies to foster young children’s self-regulation and impulse control can be incorporated into the Head Start curriculum. Finally, Head Start teachers can be taught to use basic behavior management techniques to address the needs of children with an identified externalizing problem. Family support and parent education are crucial components of any intervention to diminish behavior problems in children. The Partners Parent Program (Webster-Stratton & Herbert, 1994) is an example of a parent-focused intervention that has documented effectiveness Externalizing Problems in Head Start Children with severely oppositional preschool children. Parents need to be informed about what is normative in preschool children, and about the developmental and emotional underpinnings to young children’s negative behavior. Providing parents with concrete strategies for managing their children’s behavior also seems paramount. Learning from the structure and management strategies offered in the classroom should assist them in socializing their children at home in a more developmentally-appropriate manner. Additionally, emphasis should also be placed on improving the parents’ psychological well-being. There are multiple data sources which point to the strong relation between parent and child psychological adjustment. Thus, linking parents with adult mental health providers, assisting them to minimize the stress in their lives, and conducting activities for supporting their mental health should be central to the parent programming. In line with this, family-centered interventions which maximize family cohesion, mutual support, and emotional connections would be beneficial to parents and children alike. Fatherhood programs, which have gained some momentum in Head Start programs, should be widely implemented, with a goal of enhancing the relationship (and thus increasing the amount of time spent) between fathers and their preschool children. Home visitation would seem to be an important service delivery strategy for Head Start programs to maintain in order to address all of these family-centered issues. It is essential that Head Start produces a cadre of home visitors who are trained to deliver family support services, as well as to provide mental health intervention, specifically that which is prevention focused. Finally, assisting parents to manage the impact of larger ecological stressors (e.g., violence, poverty) on their families, as well as advocating with them for improving social conditions are Externalizing Problems in Head Start Children both central to Head Start’s family and community support and collaboration mission. Conclusions This study has expanded on previous research on behavior problems in preschoolers by investigating a population of Head Start children using a multi-modal, multi-dimensional design. The findings of the study offer empirical validation of the anecodotal reports of high rates of problematic behaviors among Head Start children. In addition, the study offers insight into child-specific and ecological factors which are associated with behavior problems in this population. Such evidence allows for a consideration of strategies that go beyond managing the “bad behavior” to those that focus on what may be at the core of children’s externalizing difficulties, such as difficult temperament, parental psychopathology, and family stress. Additionally, capitalizing on the prosocial capacities (e.g. social problem solving and positive play behaviors) of preschool children seems an important target of intervention strategies. This set of findings argues for a comprehensive approach to addressing Head Start children’s behavior problems, in which teachers, parents, and mental health professionals work in an integrated way to improve the functioning of the whole child - across developmental domains and across settings. References Achenbach, T. (1991). Manual for the Child Behavior Checklist. Burlington, VT: Externalizing Problems in Head Start Children Department of Psychiatry, University of Vermont. Achenbach, T., McConaughty, S. & Howell, C. (1987). Child/adolescent behavior and emotional problems: Implications of cross-informant correlations for situational specificity. Psychological Bulletin, 101, 213-232. Ackerman, B., Izard, C., Schoff, K., Youngsrom, E. & Kogos, J. (1999). Contextual risk, caregiver emotionality, and the problem behaviors of six- and seven-year-old children from economically disadvantaged families. Child Development, 70(6), 1415-1427. Barkley, R. (1990). Attention deficit hyperactivity disorder: A handbook for diagnosis and treatment. New York: Guilford. Behar, L. & Stringfield, S. (1974). A behavior rating scales for the preschool child. Developmental Psychology, 10(5), 601-610. Beitchman, J., Wilson, B., Brownlie, E., Walters, H., Inglis, A. & Lance, W. (1996). Long-term consistency in speech/language profiles, 2: behavioral, emotional and social outcomes. Journal of the Academy of Child and Adolescent Psychiatry, 35(6), 815-125. Bierman, K., Coie, J., Dodge, K., Greenberg, M. & McMahon, R. (in press). A developmental and clinical model for the prevention of conduct disorders: The FAST Track Program. Development and Psychopathology. Black, M., Dubowitz, H. & Starr. R. (1999). African-American fathers in low income, urban families: Development, behavior, and home environment of their three year old children. Child Development, 70(4), 967-978. Bolger, K., Patterson, C., Thompson, W. & Kupersmidt, J. (1995). Psychosocial adjustment among children experiencing persistent and intermittent family economic hardship. Externalizing Problems in Head Start Children Child Development, 66, 1107-1129. Brandt, P. & Weinart, C. (1981). The PRQ: A social support measure. Nursing Research, 30(5), 277-280. Bronfenbrenner, U. (1979). The ecology of human development: Experiments by nature and design. Cambridge, MA: Harvard University Press. Campbell, S. (1995). Behavior problems in preschool children: A review of recent research. Journal of Child Psychology and Psychiatry, 36(1), 113-149. Campbell, S. (1990). Behavior problems in preschool children. New York: Guilford. Campbell, S., March, C., Pierce, E., Ewing, L. & Szumowski, E. (1991). Hard to manage preschool boys: Family context and the stability of externalizing behavior. Journal of Abnormal Child Psychology, 19, 301-316. Crockett, L., Eggebeen, D. & Hawkins, A. (1993). Fathers’ presence and young children’s behavioral and cognitive adjustment. Journal of Family Issues, 14, 355-377. Derogatis, L. & Spencer, P. Brief Symptom Inventory: Administration, scoring, and procedures manual-I. Baltimore, MD: Clinical Psychometric Research. Dodge, K. (1993). Social-cognitive mechanisms in the development of conduct disorder and depression. Annual Review of Psychology, 44, 559-584. Downey, G. & Coyne, J. (1990). Children of depressed parents: An integrative review. Psychological Bulletin, 108(1), 50-76. Dubow, E., Tisak, J., Causey, J., Hryshko, A. & Reid, G. (1991). A two-year longitudinal study of stressful life events, social support, and social problem solving skills: Contributions to children’s behavioral and academic adjustment. Child Development, 62, 583-599. Externalizing Problems in Head Start Children Dunn, L. & Dunn, P. (1981). Peabody Picture Vocabulary Test-Revised. Circle Pines, MN: American Guidance Service. Eamon, M. (1994). Poverty and placement outcomes in intensive family preservation services. Child and Adolescent Social Work Journal, 11(5), 349-361. Eisenberg, N. & Fabes, R. (1992). Emotion, regulation, and the development of social competence. In M. Clark (Ed.), Emotion and Social Behavior: Review of Personality and Social Psychology (volume 14) (pp.119-150). Newbury Park, CA: Sage. Eisenberg, N. & Fabes, R. (1998). Prosocial development. In N. Eisenber (Eds), W. Damon (Series Ed.), Handbook of child psychology: Vol.3. Social, emotional, and personality development (5th ed., 701-778). New York: Wiley. Farrington, D. (1991). Childhood aggression and adult violence: Early precursors and later life outcomes. In D. Pepler & K. Rubin (Eds.), The Development and Treatment of Childhood Aggression (pp. 5-29). Hillsdale, NJ: Erlbaum. Fergusson, D., Lynskey, M. & Horwoood, L. (1993). The effect of maternal depression on maternal ratings of child behavior. Journal of Abnormal Child Psychology, 21, 245-270. Field, T. (1995). Psychologically depressed parents. In Bornstein, M. (Ed.), Handbook of Parenting, 4, 85-99. Mahwah, NJ: Erlbaum. Forness, S. & Finn, D. (1993). Screening children in Head Start for emotional or behavioral disorders. Severe Behavior Disorders Monograph, 16, 6-14. Forness, S., Serna, L., Kavale, K. & Nielsen, E. (1998). Mental Health and Head Start: Teaching adaptive skills. Education and Treatment of Children, 21, 258-274. Fox, N. & Leavitt, L. (1995). The Violence Exposure Questionnaire for Children Externalizing Problems in Head Start Children (Preschool Version). College Park, MD: University of Maryland. Greenberg, M., Kusche, C., Cook, E. & Quamma, J. (1995). Promoting emotional competence in school-aged children: The effects of the PATHS curriculum. Development and Psychopathology, 7, 117-136. Kazdin, A. (1995). Conduct disorders in childhood and adolescence. Thousand Oaks, CA: Sage. Keenan, K. & Shaw, D. (1997). Developmental and social influences on young girls’ behavioral and emotional problems. Psychological Bulletin, 121(1), 95-113. LaFreniere, P., Dumas, J., Capuana, F. & Dubeau, D. (1992). Development and validation of the preschool socioaffective profile. Psychological Assessment, 4, 242-250. Leadbeater, B. & Bishop, S. (1994). Predictors of behavior problems in preschool children of inner-city Afro-American and Puerto Rican adolescent mothers. Child Development, 65, 638-648. Lopez, M., Tarullo, L., Forness, S. & Boyce, C. (2000). Head Start as a venue for early identification and intervention in mental health: Implications for research and practice. Early Education and Development. Luthar, S. (1999). Poverty and children’s adjustment. In A. Kazdin (Ed.), Series on Developmental Clinical Psychology and Psychiatry, 41. Thousand Oaks, CA: Sage. Lyons-Ruth, K., Easterbrooks, M.., Davidson Cibelli, C. & Bronfman, E. (1995). Predicting school-age externalizing symptoms from infancy: Contribution of disorganized attachment strategies and mild mental lag. Presented at the biennial convention of the Society for Research in Child Development, Indianapolis, IN. Externalizing Problems in Head Start Children Lyons-Ruth, K., Alpern, L. & Repacholi, B. (1993). Disorganized infant attachment classification and maternal psychosocial problems as predictors of hostile-aggressive behavior in the preschool classroom. Child Development, 64, 572-585. Masten, A., Garmezy, N., Tellegen, A., Pellegrini, D. & Larsen, A. (1988). Competence and stress in school children: The moderating effects of individual and family qualities. Journal of Child Psychology and Psychiatry, 29, 745-764. McGee, R., Partridge, F., Williams, S. & Silva, P. (1991). A twelve-year follow-up of preschool hyperactive children. Journal of the American Academy of Child and Adolescent Psychiatry, 25, 573-586. McLoyd, V. (1998). Socioeconomic disadvantage and child development. American Psychologist, 53(2), 185-204. McLoyd, V. (1990). The impact of economic hardship on black families and children: Psychological distress, parenting, and socioemotional development. Child Development, 61, 311-346. McLoyd, V. (1998). Socioeconomic disadvantage and child development. American Psychologist, 53(2), 185-204. Meyers, H., Taylor, S., Alvy, K., Arrington, A. & Richardson, M. (1992). Parental and family predictors of behavior problems in inner-city black children. American Journal of Community Psychology, 20(5), 557-576. Moos, R. & Moos, L. (1981). Family Environment Scale. Palo Alto, CA: Consulting Psychologists Press. Office of Juvenile Justice and Delinquency Prevention (1998). Juvenile female offenders: Externalizing Problems in Head Start Children A status of the states report. Washington, DC: U.S. Department of Justice (available on the World Wide Web: http://www.ojjdp.ncjrs.org/pubs/gender/.html). Olson, S., Bates, J. & Bayles, K. (1990). Early antecedents of childhood impulsivity: The role of parent-child interaction, cognitive competence, and temperament. Journal of Abnormal Child Psychology, 18, 317-334. Osofsky, J. (1995). The effects of exposure to violence on young children. American Psychologist, 50(9), 782-788. Patterson, G. (1982). Coercive family process: Volume 3. A social learning process. Eugene, OR: Castalia Press. Patterson, G., DeBaryshe, B. & Ramsey, E. (1989). A developmental perspective on antisocial behavior. American Psychologist, 44, 329-335. Patterson, G., Reid. J. & Dishion, T. (1992). Antisocial boys. Eugene, OR: Castalia Press. Piotrkowski, C., Collins, R., Knitzer, J. & Robinson, R. (1994). Strengthening mental health services in Head Start: A challenge for the 1990's. American Psychologist, 49(2), 133-139. Raadal, M., Odont, Milgram, P., Cauce, A & Mncl, L. (1994). Behavior problems in five to eleven year old children from low-income families. Journal of American Academy of Child and Adolescent Psychiatry, 33(7), 1017-1025. Randolph, S. (1995). African-American children in single-mother families. In B. Dickerson (Ed.), African American Single Mothers. Thousand Oaks, CA: Sage. Randolph, S., Koblinsky, S., Beemer, M., Roberts, D. & Letiecq, B. (2000). Behavior problems of African American boys and girls attending Head Start programs in violent neighborhoods. Early Education and Development. Externalizing Problems in Head Start Children Raver, C., Blackburn, E., Bancroft, M. & Torp, N. (1999). Relations between effective emotional self-regulation, attentional control, and low-income preschoolers’ social competence with peers. Early Education and Development, 10(3), 333-350. Raver, C. & Zigler, E. (1997). Social competence: An untapped dimension of Head Start’s success. Early Childhood Research Quarterly, 12, 363-385. Richters, J. (1992). Depressed mothers as informants about their children: A critical review of the evidence for distortion. Psychological Bulletin, 112(3), 485-499. Richters, J. & Martinez, P. (1993). Violent communities, family choices, and children’s changes: An algorithm for improving the odds. Development and Psychopathology, 5, 609-627. Rothbart, M. & Bates, J. (1998). Temperament. In N. Eisenberg (Ed.), W. Damon (Series Ed.), Handbook of Child Psychology: Vol.3. Social, emotional, and personality development (5th ed., 105-176). New York: Wiley. Rowe, P. & Plomin, R. (1977). Colorado Child Temperament Inventory. Denver, CO: University of Colorado. Rubin, K. (1988). Social Problem Solving Test - Revised. Waterloo, CA: University of Waterloo. Rubin, K., Bream, L. & Rose-Krasnor, L. (1991). Social problem solving and aggression in childhood. In D. Pepler & K. Rubin (Eds.), The Development and Treatment of Childhood Aggression (219-248). Hillsdale, NJ: Erlbaum. Rubin, K., Coplan, R., Fox, N. & Calkins, S. (1995). Emotionality, emotion regulation, and preschooler’s social adaptation. Development and Psychopathology, 7, 49-62. Rubin, K. & Rose-Krasnor, L. (1986). Interpersonal problem-solving and social Externalizing Problems in Head Start Children competence in young children. In V. Van Hasselt & M. Hersen (Eds.), Handbook of social development: A lifespan perspective (283-323). New York: Plenum. Rutherford, R., Quinn, M. & Mathur, S. (1995). Effective strategies for teaching appropriate behaviors to children with emotional/behavioral disorders. Reston, VA: Council for Exceptional Children. Sanson, A., Smart, D., Prior, M. & Oberklaid, F. (1993). Precursors of hyperactivity and aggression. Journal of the American Academy of Child and Adolescent Psychiatry, 32(6), 12071216. Shahinfar, A., Fox, N., Leavitt, L., & Richters, J. (in press). Preschool children’s exposure to violence: Relations between parent and child perceptions of prevalence and behavior problems. American Journal of Orthopsychiatry. Shaw, D., Owens, E., Vondra, J., Keenan, K. & Winslow, E. (1996). Early risk factors and pathways in the development of early disruptive behavior problems. Development and Psychopathology, 8, 679-699. Shure, M. & Spivak, G. (1980). Interpersonal problem-solving as a mediator of behavioral adjustment in preschool and kindergarten children. Journal of Applied Developmental Psychology, 1, 29-44. Sinclair, E., DelHomme, M. & Gonzalez, M. (1993). Systematic screening for preschool behavioral disorders. Journal of Behavioral Disorders, 18(3), 177-188. Tremblay, P. (1991). Commentary - Aggression, prosocial behavior, and gender: Three magic words, but no magic wand. In D. Pepler & K. Rubin (Eds.), The Development and Treatment of Childhood Aggression (219-248). Hillsdale, NJ: Earlbaum. Externalizing Problems in Head Start Children Tremblay, R., Pihl, R. Vitaro, F. & Dobkin, P. (1994). Predicting early onset of male antisocial behavior from preschool behavior. Archives of General Psychiatry, 51, 732-739. Tynan, W. & Nearing, J. (1994). The diagnosis of attention deficit hyperactivity disorder in young children. Infants and Young Children, 6(4), 13-20. Walker, H., Colvin, G. & Ramsey, E. (1995). Antisocial behavior in school: Strategies and best practices. Longmont, CO: Sopris West. Walker, H., Kavanagh, K., Stiller, B., Golly, A., Severson, H. & Feil, E. (1998). First Step to Success: An early intervention approach for preventing school antisocial behavior. Journal of Emotional and Behavioral Disorders, 6(2), 66-80. Webster-Stratton, C. (1989). The relationship of marital support, conflict, and divorce to parent perceptions, behaviors, and childhood conduct problems. Journal of Marriage and the Family, 51, 406-416. Webster-Stratton, C. (1985). The effects of father involvement in parent training for conduct problem children. Journal of Child Psychology and Psychiatry, 26, 801-810. Webster-Stratton, C. & Hammond, M. (1998). Conduct problems and level of social competence in Head Start children: Prevalence, pervasiveness, and associated risk factors. Clinical Child and Family Psychology Review, 1(2), 101-123. Webster-Stratton, C. & Hammond, M. (1988). Maternal depression and its relationship to life stress, perceptions of child behavior problems, parenting behaviors, and child conduct problems. Journal of Abnormal Child Psychology, 16, 299-315. Webster-Stratton, C. & Herbert, M. (1994). Troubled families - problem children. New York: Wiley. Externalizing Problems in Head Start Children Weintraub, M. & Gringlas, M. (1995). Single parenthood. In M. Bornstein (Ed.), Handbook of parenting: Volume 3. Status and social conditions of parenting (65-87). Mahwah, NJ: Lawrence Erlbaum. Wilson, B. (1999). Entry behavior and emotion regulation abilities of developmentally delayed boys. Developmental Psychology, 35, 214-222. Yoshikawa, H. & Knitzer, J. (1997). Lessons from the field: Head Start mental health strategies to meet changing needs. New York: National Center for Children in Poverty. Zahn-Waxler, C., Iannotti, R., Cummings, E. & Denham, S. (1990). Antecedents of problem behaviors in children of depressed mothers. Development and Psychopathology, 2, 271291. Zahn-Waxler, C., Klimes-Dougan, B. & Slattery, M. (in press). Internalizing problems of childhood and adolescence: Prospects, pitfalls, and progress in understanding the development of anxiety and depression. In D. Cicchetti & A. Sroufe (Eds.), Millenium Special Issue on Development and Psychopathology, Development and Psychopathology. Zigler, E., Taussig, C. & Black, K. (1992). Early childhood intervention: A promising preventative for juvenile delinquency. American Psychologist, 47, 997-1006. Zimmerman, M., Salem, D. & Maton, K. (1995). Family structure and psychosocial correlates among urban African-American adolescent males. Child Development, 66, 15981613. Zocolillo, M. (1992). Co-occurrence of conduct disorder and its adult outcomes with depressive and anxiety disorders: A review. Journal of the American Academy of Child and Adolescent Psychiatry, 31, 547-556. Externalizing Problems in Head Start Children Externalizing Problems in Head Start Children Figure Captions Figure 1 - Proportion of Girls (n=76) with Externalizing Behavior in the Normal (68.4%; n=52), Borderline (10.5%; n=8), and Clinical (21.1%; n=16) Ranges Figure 2 - Proportion of Boys (n=79) with Externalizing Behavior in the Normal (84.8%; n=87), Borderline(5.1%; n=4), and Clinical (10.1%; n=8) Ranges Externalizing Problems in Head Start Children Externalizing Problems in Head Start Children Table 1 Sample Characteristics: Primary Caregiver of Child (n=155) Externalizing Problems in Head Start Children ______________________________________________________________________________ Characteristic Proportion ______________________________________________________________________________ Relationship to child Biological Mother 88.4% Biological Father 2.6% Grandmother 6.5% ______________________________________________________________________________ Religion Baptist 56.6% Catholic 15.0% None 10.4% ______________________________________________________________________________ Race/Ethnicity African-American 98.8% Asian 0.6% Bi-racial 0.6% ______________________________________________________________________________ Highest grade completed <High School 25.8% High School/GED 51.6% Some post high school 22.6% ______________________________________________________________________________ Employment status Unemployed 69.7% Part-time 15.5% Full-time 14.8% ______________________________________________________________________________ Marital status Single/separated 81.2% Married to child’s parent 11.0% Married to another 7.8% ______________________________________________________________________________ Table 2 Means and Standard Deviations for Child and Parent Characteristics for Total Sample (N=155) and Externalizing Group (n=42) Externalizing Problems in Head Start Children _______________________________________________________________ Characteristic Total Sample Externalizing M SD M SD _______________________________________________________________ CBCL Externalizing 10.9 6.4 20.5 3.8 CBCL Internalizing 4.5 0.4 7.6 5.0 CTI Emotionality 2.6 0.9 3.4 0.7 CTI Activity 4.1 0.7 4.1 0.7 CTI Attention 3.4 1.3 3.1 0.8 CTI Soothability 3.8 0.7 3.6 0.7 CTI Shyness 2.3 0.8 2.2 0.8 62.7 17.9 64.4 20.1 BSI Total 6.2 5.4 7.3 5.0 BSI Depression 0.4 0.7 0.6 0.6 BSI Hostility 0.4 0.5 0.8 0.7 BSI Symptom Distress 1.6 0.7 2.0 0.6 FES Conflict 2.8 1.9 3.6 2.1 FES Expressiveness 5.2 1.7 5.0 1.8 FES Cohesion 7.3 1.7 7.0 1.6 FES Organization 6.6 1.8 6.3 2.0 PPVT Receptive Vocabulary VEX-P Violence Exposure 2.0 2.0 3.1 2.4 _______________________________________________________________ Table 3 Intercorrelations Between Child-Specific Variables and Externalizing Behavior (n=155) Externalizing Problems in Head Start Children ______________________________________________________________________________ Variable 1 2 3 4 5 6 7 8 9 ______________________________________________________________________________ 1. Externalizing 1.00 2. Internalizing .53***-- 3. Emotionality .55***.48 4. Activity .08 -.13 --.06 -- 5. Attention -.23**-.14 -.21* .08 -- 6. Soothability -.17* -.07 -.18* .20* .11 7. Shyness -.13 8. Dysregulation .28** .14 -.40** -.03 .49***.39** .82***-.16* --.17* -- -.21* -.71*** .20* -- 9. PPVT .04 .01 .08 .20* -.01 -.09 -.06 .10 1.00 ______________________________________________________________________________ * p<.05 ** p<.01 ***p<.001 Table 4 Intercorrelations Between Ecological Variables and Externalizing Behavior (n=155) ______________________________________________________________________________ Variable 1 2 3 4 5 6 7 8 9 10 ______________________________________________________________________________ 1. Externalizing 1.00 2. BSI Global Symptoms 3. BSI Depression 4. BSI Hostility 5. BSI Symptom Distress 6. FES Conflict 7. FES Expressiveness 8. FES Cohesion 9. FES Organization .45*** .29** .50***.32*** .29** -.02 -.14 -.18* .31** -- .84***.68*** .57***.27** -.14 -.37** -.20* .30** -- -.41 .48** * .43** .20* -- -.13 -.12 .13 .39** .28** -.10 -.23** -.31** .27** -- -.28** -.14 .22** -.14 -- -.16 -- .21* -.50***-.38** .23* .32** .15 -- .12 .31** -.09 -- -.08 10. Violence Exposure 1.00 ______________________________________________________________________________ *p<.05 **p<.01 Table 5 Means and Standard Deviations for Observed Behaviors Among Externalizing Group (n=42) ____________________________________________________________ Observed Behavior M SD ____________________________________________________________ Appropriate Behaviors 80.35 7.97 Solitary Play 4.17 4.37 Group Play 11.58 8.50 Dramatic Play 3.54 4.95 Rough-and-Tumble Play 1.10 2.76 On-Task Behavior 59.97 14.24 19.54 8.17 Hyperactive-Impulsive Behavior 13.44 7.53 Withdrawn Behavior 4.58 4.60 Aggressive-Initiating Behavior 0.81 0.93 Aggressive-Reactive Behavior 0.29 0.63 Inappropriate Behaviors Negative Affect 0.42 1.37 ____________________________________________________________ Table 6 Intercorrelations Between Social Problem Solving and Teacher Ratings of Behavior Problems (n=40) ______________________________________________________________________________ Socially Anxious Hyperactive Hostile Social Problem Solving Competent Fearful Distractible Aggressive ______________________________________________________________________________ Prosocial Strategies .13 -.56** -.36* -.10 Agonistic Strategies -.06 .03 .21 -.01 Trade/Bribe Strategies -.08 .29 .06 -.03 Inappropriate Strategies .32 .33 .24 -.22 Manipulate Affect Strategies -.18 .27 .17 .15 Authority Strategies -.01 .44** -.05 -.12 Flexibility -.06 -.39* -.24 -.28 Relevancy -.08 -.37* -.28 -.34* ______________________________________________________________________________ *p<.05 **p<.01 HEAD START AND MENTAL HEALTH: A FERTILE FIELD FOR PRACTICE AND RESEARCH Preface to the Special Issue For over three decades, Head Start has been a national laboratory for inquiry into the functioning and experiences of young children from low-income backgrounds (Zigler & Valentine, 1997). Research involving Head Start children, families, and programs has become one of the best exemplars of the use of applied developmental research for informing policy (Zigler & Styfco, 1993). Although some scholars have criticized the use of this evidence as the basis for our knowledge of minority child development (e.g., Washington & Oyemade, 1987), Head Start research initiatives continue to be the primary source of data on the needs and competencies of young children in impoverished minority families. The proliferation of studies on Head Start children in the last few decades has generated a large body of evidence on participant children’s cognitive and academic functioning, but comparatively little on their social competence and mental health (Raver & Zigler, 1997; Yoshikawa & Knitzer, 1997). Despite the identification of child social competence as the overall goal of Head Start programs, and in spite of the regulatory mandate to address the mental health needs of participant children (Head Start Program Final Rule, 1996), the mental health and social competence of Head Start children remain underexplored. Because of the documented association between low socioeconomic status and psychological difficulties, the Head Start program presents the research community with a unique opportunity to expand the knowledge base about the prevalence of mental health problems and the factors that contribute to emotional functioning in this segment of the preschool population. Although children’s mental health is receiving more attention from clinical and research perspectives, there is still a paucity of data relevant to the mental health functioning of young children from impoverished backgrounds, such as those in Head Start. This lack of knowledge in the field as a whole presents a clear rationale for incorporating a mental health focus in empirical investigations involving Head Start. Another rationale for exploring mental health issues in Head Start emanates directly from the experiences of participant children and teachers. In their investigation of the mental health strategies employed in Head Start programs, Yoshikawa and Knitzer (1997) cite the increasing levels of stress encountered by Head Start children in their home environments, and the mounting reports by Head Start staff of escalating behavior problems in participant children. Both these issues have led to a renewed emphasis on identifying and intervening with children with psychological difficulties. Similarly, scholars and practitioners have called for an increase in research investigating which mental health interventions are most effective for specific populations and particular mental health issues (O’Brien, 1994). The goal of this special issue is to present and integrate current knowledge about the mental health needs of Head Start children. Accordingly, papers have been selected which address historical and current trends in Head Start mental health services, the prevalence of mental health problems in Head Start children, andchild-specific and environmental influences on the psychological functioning of these children. Through this exploration of this specific group of children, papers in this special issue contribute to the understanding of emotional problems in young children as well as inform policy and programmatic initiatives designed to address the mental health needs of children in the Head Start population. Three papers in this issue approach the subject of mental health broadly, from programand system-level perspectives. First, Yoshikawa and Zigler explore the historical and future landscape of mental health in Head Start. They consider some of the major challenges of maintaining a focus on mental health in a 21st century Head Start program, including definitional issues, program-level services, system level coordination, and macro-level policy factors. Lopez and colleagues use program information reports (PIR’s) to provide national data on the numbers of children identified with emotional problems in all Head Start programs. These data are contextualized with a thoughtful discussion of prevalence evidence from other research initiatives, including studies of individual programs and from other sources such as parents. Lara, McCabe and Brooks-Gunn offer a qualitative exploration of the strategies employed by Head Start staff in 5 different centers to deliver mental health services. They discuss the role of management style in how teachers and other staff intervene with children and families who present with emotional difficulties. The remainder of the papers in this special issue examine the characteristics of participant children and families relevant to their mental health. Fagan and Iglesias investigate an often ignored area of research - the contribution of fathers to children’s developmental outcomes. Specifically, they address the influence of father’s communication styles on children’s language and behavioral competence. Koblinsky, Gordon and Anderson explore the functioning of Head Start children experiencing homelessness. They compare the social skills and behavior problems of homeless and housed children at two points during the Head Start year. Two studies address individual and ecological influences on behavioral problems in Head Start children. Randolph and colleagues investigate the role of gender and community violence on the existence of behavioral problems in Head Start children. Jones Harden and colleagues address several factors in their investigation of externalizing behaviors in Head Start children, including individual characteristics such as gender, cognition, and temperament, and ecological issues such as parental characteristics, family environment, and community violence. This study explores the relation between parent-identified behavioral problems and children’s presentation of socially competent or behavioral difficulties in the classroom. This special issue is devoted to understanding mental health issues affecting children who participate in Head Start, as well as exploring programs’ delivery of mental health services. The papers individually and collectively amplify the magnitude of the gap between policy, practice, and research in the mental health domain. Several specific directions for practice and research have emerged from the analyses presented here. Addressing infrastructure issues, Yoshikawa and Zigler call for increased program incentives and enhanced training and technical assistance efforts in providing mental health services through Head Start. Lara, McCabe and Brooks-Gunn highlight the importance of infusing a mental health focus in staffing, supervision, and management strategies. Consistent with the comprehensive program philosophy of Head Start, the paper by Jones Harden and colleagues suggests that mental health services in Head Start should address the needs of children and families, through classroom-based and home-based interventions at the preventive and targeted levels. Fagan and Iglesias point to the importance of providing targeted support to fathers in family-centered interventions. Finally, the papers by Koblinsky et al. and Randolph et al. underscore that interventions must address the external stressors that impinge upon mental health functioning, such as homelessness and community violence. Research directions for Head Start and mental health have been described richly and succinctly by Lopez, Tarullo, Forness and Boyce. They describe a new generation of collaborative research which includes careful evaluation of sophisticated program designs. Further, they delineate five key areas for future research: “1) population prevalence estimates and developmental trajectories for young children’s mental health problems; 2) new measures and methodologies for assessing developmental psychopathology; 3) cost-effective approaches to early identification, prevention, and intervention; 4) improved understanding of mental health service utilization patterns; and 5) better approaches to implementing high quality, communitybased systems of care”. Given the ascendancy of interest in early intervention in current political, funding, and research circles, the time is ripe for programmatic and empirical initiatives on mental health in Head Start populations. The paradoxical situation in which Head Start scholars and practitioners find themselves is one in which mental health services are mandated but do not yet receive the national or individual program emphasis that they should. Resultant gaps in program and research implementation around mental health issues create fertile soil for generating new knowledge about the mental health functioning of children in poverty, as well as effective intervention strategies to promote their optimal mental health. The authors, reviewers and editorial board and staff who invested time and energy in this special issue hope that we have contributed to moving the mental health of Head Start children to a place of prominence for policy-makers, practitioners, and researchers. Brenda Jones Harden References Campbell, S. (1995). Behavioral problems in preschool children: A review of recent research. Journal of Child Psychology and Psychiatry, 36(1), 113-149. Head Start Program Final Rule, 45 CFR § 1301 (1996). O’Brien, James. (1994). Head Start and mental health (special issue). National Head Start Bulletin, 49. Raver, C. & Zigler, E. (1997). Social competence: An untapped dimension of Head Start’s success. Early Childhood Research Quarterly, 12, 363-385. Washington, V. & Oyemade, U. (1987). Project Head Start: Past, present and future trends in the context of family needs. New York: Garland. Yoshikawa, H. & Knitzer, J. (1997). Lesons from the field: Head Start mental health strategies to meet changing needs. New York: National Center for Children in Poverty. Zigler, E. & Styfco, S. (1993). Using research and theory to justify and inform Head Start expansion. Society for Research in Child Development Social Policy Report, 7(2). Zigler, E. & Valentine, J. (Eds.)(1997). Project Head Start: A legacy of the War on Poverty (2nd edition). Alexandria, VA: National Head Start Association.