Patient Review of Systems
advertisement

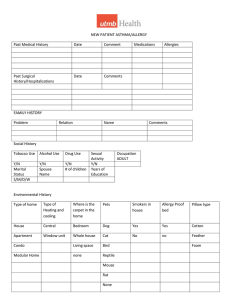
Patient Name: __________________________________ Date: ____________________ Please circle any symptoms that you or your child has experienced: General Fevers Chills Sweats Fatigue Weight loss Musculoskeletal Back pain/muscle pain Joint swelling Joint pain Cramping Weakness Genitourinary Frequency of urination Pain with urination Blood in urine Discharge Eyes Redness Discharge Eye pain Itchy Watery Vision loss Irritation Dryness Nose Congestion Runny nose Post nasal drip Nose bleeds Itching Sneezing Gastrointestinal Heartburn Nausea Vomiting Diarrhea Difficulty swallowing Abdominal pain Bloody stools Ears Earache Drainage Ringing in ear Decreased hearing Fullness Itching Throat Hoarseness Throat fullness Sore throat Throat clearing/drainage Itching Throat swelling Skin Swelling Hives Rash Itching Dryness Bruising Eczema Mental Health Depression Anxiety Behavioral changes Hyperactivity Cardio Chest pains Palpitations Passing out High blood pressure Neurological Headache Dizziness Seizures Memory loss Endocrine Intolerance to Hot and Cold Facial flushing Increased thirst Respiratory Cough Chest tightness Wheezing Shortness of breath Sputum Production Allergy/Immunology Recurrent infections Insect sting allergy Food allergy