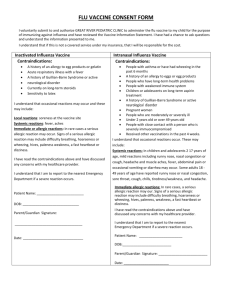
The Caring Van is offering children free flu shots who qualify for the
advertisement

Child’s Name: __________________________________________ Teacher/Grade/Classroom#: ______________________________ The Oklahoma Caring Van is offering free flu vaccine to children who qualify for the Vaccines for Children (VFC) Program. In order for your child to qualify for the VFC program, one of the following criteria must be satisfied. Please check all of the following that apply. (At least one box must be checked to receive vaccine): □ My child is covered through Soonercare/Medicaid #____________ □ My child is Native American. □ My child is Native Alaskan, Native Hawaiian or other Pacific Islander. □ My child does not have private insurance. If you checked any of the items above, please mark your preference below: □ I would like my child to receive the flu injection only. □ I would like my child to receive the flu mist only. □ My child may have the flu injection or flu mist, whichever is available. Screening Questions for Inactivated (Shot) Flu Vaccine 1. Has your child ever had an influenza vaccine? 2. Has your child ever had a bad reaction to the influenza vaccine? If “yes” what was the reaction?__________________ 3. Does your child have a fever, infection or current illness today? If “yes” what illness? __________________________ 4. Is your child allergic to chicken eggs, latex, thimerosal or gelatin? If “yes” what kind of reaction? __________________ 5. Has your child experienced Guillain-Barre syndrome? Yes Yes No No Yes No Yes No Yes No Screening Questions for Live Nasal (mist) Influenza Vaccine Note: If your child has had wheezing or asthma in the last year nasal mist can NOT be given 1. Is your child pregnant? Yes No 2. Is the patient between 2 and 4 years of age and has wheezing or asthma? Yes No 3. Does your child have long term health problems with heart, lung, kidney, etc.? Yes No 4. Is the patient a child or adolescent on long-term aspirin treatment? Yes No 5. Has your child had one or more episodes of wheezing in the past year? Yes No 6. Does your child have allergic reaction to egg, arginine, gentamicin, and/or gelatin? Yes No If “yes” describe __________________________ 7. Is your child currently taking antiviral medication or have taken in the last 48 hours? Yes No If “yes” what medication _____________________ 8. Has the person to be vaccinated received any other vaccinations in the past 4 weeks? Yes No If “yes” what vaccinations?_____________________ 9. Does your child have a weakened immune system or do you live with anyone who does? Yes No If “yes what___________ Do they live in the home with you? ________