Article 107 checklist
advertisement

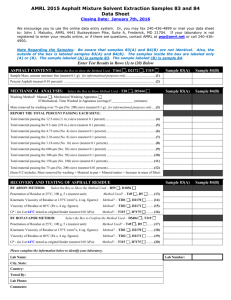
Office of Care and Protection Patients’ Office ARTICLE 107 CHECKLIST Patient’s details □ Full name □ Present address □ Previous address(es) □ Date of birth □ National Insurance number □ Marital status □ Former occupation(s) □ Confirmation if Patient ever granted Power of Attorney / Enduring Power of Attorney to anyone, and if so, that person’s details □ A Medical Certificate [e.g. Form F5] must be attached to the Article 107 Referral Notice Nearest Relative details □ Name □ Address □ Telephone number □ Relationship to Patient □ Has Notice been given to the nearest relative [Article 108(2)] □ Is the nearest relative willing / suitable to act on behalf of Patient □ If not, provide details of another relative / friend who is willing to act Financial details [list all income, assts and property] □ Bank / Building Society / Post Office accounts (including account name and address, account number, and present balance) □ Investments (including name and address of whom investment held with, reference numbers, and present value) □ State or occupation pensions / benefits / direct payments (including amount, frequency of payment, and where it is being paid to) □ Details of private pensions (including name and address of payer, amount, frequency of payment, and where it is being paid to) □ Any interest in a dwelling house [is house secure? Is house insured?] □ Any interest in any other properties, lands or stock □ Significant personal effects or other valuable assets □ Outstanding debts and recurring charges □ Details of any Solicitor acting on behalf of the Patient or family [or any Solicitor who has previously acted if no one currently acting] □ Confirm the whereabouts of the Patient’s title deeds, will, cash and jewellery Action □ What action or intervention do you require OCP to take? □ What urgent action is required by the Court [e.g. freeze bank accounts, insure or secure premises, protect valuables, arrange a visit to the Patient, seek a Court direction or Order etc.] Date: Signed: Position / Qualification: Print name: Address: Telephone No: Email: Please note Should difficulties be encountered in attempting to establish any of the above information the Office can issue an appropriate person [such as a Trust Official] with Court authority to investigate a Patient’s financial affairs. 9-9-11