Pretransplant Dialysis Duration and Risk of Death After Kidney
advertisement

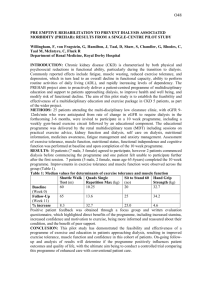
H-14: transplant monitoring H-15: late rejection F-05: conventional hemodialysis Pretransplant Dialysis Duration and Risk of Death After Kidney Transplantation in the Current Era Helanterä, Ilkka1,4; Salmela, Kaija2; Kyllönen, Lauri2; Koskinen, Petri1; Grönhagen-Riska, Carola1,3; Finne, Patrik1,3 Transplantation: 27 August 2014 - Volume 98 - Issue 4 - p 458-464 Author Information 1 Department of Medicine, Division of Nephrology, Helsinki University Central Hospital, Helsinki, Finland. 2 Department of Transplant Surgery, Helsinki University Central Hospital, Helsinki, Finland. 3 Finnish Registry for Kidney Diseases, Helsinki, Finland. 4Address correspondence to: Ilkka Helanterä M.D., Ph.D, Department of Medicine, Division of Nephrology, Helsinki University Hospital, Haartmaninkatu 4, Helsinki, Finland. E-mail: ilkka.helantera@helsinki.fi ABSTRACT Background Although longer pretransplant dialysis has been associated with poor kidney transplant outcome, no data about this association exist from the current era or from Europe. We studied the association of pretransplant dialysis duration on outcomes after kidney transplantation across two different time periods. Methods All recipients of first kidney transplantation between 1990 and 2010 in Finland were included (N=3,105) in this observational follow-up study of an inception cohort. The association of the duration of pretransplant dialysis with patient and graft survival after transplantation was analyzed with multivariable Cox regression and competing risk analyses. The association of pretransplant dialysis duration with the risk of specific causes of death (cardiovascular, infectious, or other) was analyzed using competing risk analysis. Results Longer duration of pretransplant dialysis was an independent risk factor for patient death after transplantation (risk ratio [RR] 1.14 per 1-year increase) in the whole study population, but not for graft loss. Risk of death was increased in patients with greater than 12 months of pretransplant dialysis. After further adjustment in patients transplanted in 2000 to 2010, longer duration of dialysis remained an independent risk factor (RR 1.23 per 1-year increase). Longer duration of dialysis was an independent predictor of death resulting from cardiovascular diseases (RR 1.14 per 1-year increase), but not for other causes. Conclusions The risk of death associated with longer duration of dialysis has not decreased over time, but remains an independent predictor of patient death after kidney transplantation because of increased risk of death resulting from cardiovascular diseases. COMMENTS The aim of this nationwide study was to investigate whether the association of pretransplant dialysis duration with outcomes after kidney transplantation has changed over time, and whether the association still remains in the current era. In addition, the aim was to study the association of pretransplant dialysis duration with specific causes of death. The inception cohort of this study included all recipients of first kidney transplantation in Finland between 1990 and 2010 (N=3105). Patients were followed until death (also after graft loss) or December 31, 2010. Data were obtained from the Finnish Registry for Kidney Diseases, In multivariable Cox proportional hazards model, pretransplant dialysis duration (risk ratio, RR 1.14 per 1-year increase) was an independent risk factor for patient death after transplantation When duration of pretransplant dialysis was categorized in an otherwise similar model, 6 to 11 months of dialysis before transplantation was not associated with higher risk of death compared to 0 to 5 months of dialysis (RR 1.05, 95% confidence interval 0.93–1.18, P=0.46), whereas 12 to 23 months of dialysis (RR 1.18, 95% CI 1.05–1.33, P=0.007), 24 to 35 months of dialysis (RR 1.22, 95% CI 1.04–1.43, P=0.02), 36 to 59 months of dialysis (RR 1.37, 95% CI 1.13–1.68, P=0.002), and more than 60 months of dialysis (RR 2.10, 95% CI 1.54–2.56, P<0.001) were all associated with higher risk for death compared to 0 to 5 months of dialysis. Increased duration of pretransplant dialysis was associated only with the risk of cardiovascular death (RR 1.14 per 1-year increase). Increased duration of pretransplant dialysis was not a significant independent risk factor for death resulting from infections or other causes In conclusion, longer duration of pretransplant dialysis is associated with increased risk of death after transplantation also in the current era, because of increased risk of death resulting from cardiovascular disease. The risk associated with longer duration of dialysis has not decreased over time. These results support the ongoing efforts to increase rapid access to waiting list and transplantation in patients who start maintenance dialysis. Pr. Jacques CHANARD Professor of Nephrology