Strahlenther Onkol - hem
advertisement

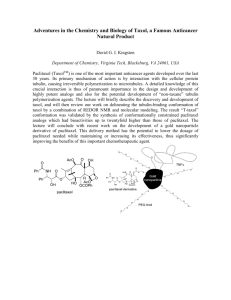
J Neurooncol. 2004 Oct;70(1):91-5. Phase II study of concurrent continuous Temozolomide (TMZ) and Tamoxifen (TMX) for recurrent malignant astrocytic gliomas. Spence AM, Peterson RA, Scharnhorst JD, Silbergeld DL, Rostomily RC. Departments of Neurology, University of Washington School of Medicine, Seattle, WA 98195, USA. aspence@u.washington.edu PURPOSE AND BACKGROUND: The aim of this study was to assess the frequency of response and toxicity in adults with recurrent anaplastic astrocytoma (AA) or glioblastoma multiforme (GM) treated with concurrent continuous TMZ and TMX. METHODS: In addition to histology, eligibility included age > 18 years, Karnovsky score > or = 60, normal laboratory parameters, no radiotherapy (RT) for 4 weeks, measurable disease and normal EKG. The chief exclusions were: previous TMZ, TMX or dacarbazine (DTIC); nitrosourea within 6 weeks; history of deep venous thrombosis or pulmonary emboli. All patients (pts) had received prior RT. TMZ was given at 75 mg/M2/day for 6 weeks, repeated every 10 weeks, maximum 5 cycles. Four pts received 60 mg/M2/day for 6 weeks due to extensive prior chemotherapy exposure. TMX was started at 40 mg twice daily (b.i.d.) for 1 week and then was increased in three successive weeks to 60, then 80, then 100 mg b.i.d. Response was assessed before every cycle with MRI +/- gadolinium (Gd). RESULTS: Sixteen pts enrolled: GM 10, AA 6; female 6, male 10; median age 48 (21-58); prior chemotherapy 7. There was one partial response and one stable disease. Eleven pts progressed by the end of cycle 1; three pts failed due to toxicity before completing cycle 1. Median time to treatment failure was 10 weeks. The main toxicities were: transaminitis, pancytopenia, 1st division herpes zoster, deep vein thrombosis and fatigue. The study was closed due to the low response rate and frequency of toxicity. J Control Release. 2004 Sep 30;99(2):259-69. Paclitaxel nanoparticles for the potential treatment of brain tumors. Koziara JM, Lockman PR, Allen DD, Mumper RJ. Division of Pharmaceutical Sciences, Center for Pharmaceutical Science and Technology, College of Pharmacy, University of Kentucky, 725 Rose Street, Lexington, KY 40536-0082, USA. Despite the advances in tumor therapy, patients with primary brain tumors and brain metastases have a very poor prognosis. Low responses to chemotherapy are mainly attributed to impermeability of the blood-brain barrier to cytotoxic agents. Paclitaxel has been shown to be active against gliomas and various brain metastases. However, its use in treatment of brain tumors is limited due to low blood-brain barrier permeability and serious side effects associated with administration of the paclitaxel solvent, Cremophor EL. Lack of paclitaxel brain uptake is thought to be associated with the p-glycoprotein (p-gp) efflux transporter. In this work, paclitaxel (PX) was entrapped in novel cetyl alcohol/polysorbate nanoparticles. Paclitaxel nanoparticles (PX NPs) were characterized by means of size, short-term stability, drug entrapment efficiency, and release profile. The PX NP cytotoxicity profile was monitored using two different cell lines, U-118 and HCT-15. Brain uptake of PX NPs was evaluated using an in situ rat brain perfusion model. The results suggest that entrapment of paclitaxel in nanoparticles significantly increases the drug brain uptake and its toxicity toward p-glycoprotein expressing tumor cells. It was hypothesized that PX NPs could mask paclitaxel characteristics and thus limit its binding to p-gp, which consequently would lead to higher brain and tumor cell uptake of the otherwise effluxed drug. J Mol Neurosci. 2003;20(3):339-43. Overcoming the blood-brain barrier to taxane delivery for neurodegenerative diseases and brain tumors. Rice A, Michaelis ML, Georg G, Liu Y, Turunen B, Audus KL. Department of Pharmaceutical Chemistry, University of Kansas, 226 Simons, 2095 Constant Avenue, Lawrence, KS 66047, USA. The blood-brain barrier (BBB) effectively prevents microtubule (MT)-stabilizing drugs from readily entering the central nervous system (CNS). A major limiting factor for microtubule-stabilizing drug permeation across the BBB is the active efflux back into the circulation by the overexpression of the multidrug-resistant gene product 1 (MDR1) or Pglycoprotein (P-gp). This study has focused on strategies to overcome P-gp-mediated efflux of Taxol analogs, MT-stabilizing agents that could be used to treat brain tumors and, potentially, neurodegenerative diseases such as Alzheimer's disease. However, taxol is a strong P-gp substrate that limits its distribution across the BBB and therapeutic potential in the CNS. We have found that addition of a succinate group to the C-10 position of paclitaxel (Taxol) results in an agent, Tx-67, with reduced interactions with Pgp and enhanced permeation across the BBB in both in vitro and in situ models. Our studies demonstrate the feasibility of making small chemical modifications to Taxol to generate analogs with reduced affinity for the P-gp but retention of MT-stabilizing properties, i.e., a taxane that may reach and treat therapeutic targets in the CNS. Clin Cancer Res. 2003 Aug 15;9(9):3441-7. Polilactofate microspheres for Paclitaxel delivery to central nervous system malignancies. Li KW, Dang W, Tyler BM, Troiano G, Tihan T, Brem H, Walter KA. Department of Neurosurgery, Johns Hopkins University School of Medicine, Baltimore, Maryland 21205, USA. PURPOSE: The purpose of this study was to demonstrate that surgically implanted, controlled-release, biodegradable polilactofate microspheres (Paclimer) can be used safely to bypass the blood-brain barrier and deliver paclitaxel to malignant brain tumors. EXPERIMENTAL DESIGN: The rate of paclitaxel release from Paclimer microspheres submerged in PBS was measured in vitro by high-performance liquid chromatography. In vivo studies of Paclimer were performed as intracranial implants in Fischer 344 rats in the presence or absence of 9L gliosarcoma. Mantel-Cox statistics were used to assess the efficacy of Paclimer at extending survival of tumor-bearing animals compared with control implants. Paclimer implants tagged with [(3)H]paclitaxel were used to measure biodistribution of paclitaxel from the Paclimer implant. RESULTS: Paclimer released paclitaxel at a constant rate for up to 3 months in vitro. In vivo, Paclimer implants placed intracranially in rats released active drug for up to 30 days after implantation and doubled the median survival of rats bearing established 9L gliosarcomas (median survival of paclitaxel-treated animals = 35 days; median survival of control-treated animal = 16 days; P < 0.0001). Active drug was distributed throughout the rat brain based on liquid scintillation counting and TLC. Rats implanted with Paclimer demonstrated no overt signs of neurotoxicity and exhibited local cytopathological changes consistent with exposure to an antimicrotubule agent. CONCLUSIONS: Paclimer extends survival in a rodent model of glioma with minimal morbidity and optimal pharmacokinetics. Anticancer Drugs. 2003 Jul;14(6):417-22. Population pharmacokinetics of low-dose paclitaxel in patients with brain tumors. Hempel G, Rube C, Mosler C, Wienstroer M, Wagner-Bohn A, Schuck A, Willich N, Boos J. Klinik und Poliklinik fur Kinderheilkunde (Padiatrische Hamatologie/Onkologie), Munster, Germany. hempege@uni-muenster.de Our aim was to assess the pharmacokinetics of a low-dose schedule of paclitaxel in combination with radiation therapy in patients with brain tumors. Eighteen patients received 20-50 mg/m2 paclitaxel as a 1-h infusion 18-24 h before radiation with 2 Gy on 5 consecutive days. In total, 156 plasma samples from 13 patients and 38 urine samples from nine patients were collected and analyzed by a validated capillary electrophoresis method. Data analysis was done using NONMEM with a two-compartmental model and proportional error model. No signs of non-linearity in the pharmacokinetic parameters were observed in this dosing range. The median cumulative urinary excretion was 2.4% (range 0.86-7.72%) of the given dose. Plasma clearance was found to be 6.71 l/h+/-70% and central volume of distribution was 3.64 l+/-79% (population mean +/- interindividual variability, respectively). At the time of the radiation, i.e. 24 h after administration with the lowest dose of 20 mg/m2, the mean concentration of paclitaxel was 0.038 mg/l (0.045 microM) in plasma. We conclude that even with the lowest dose of 20 mg/m2 paclitaxel, plasma concentrations at the time of radiation are achieved which are radiosensitizing in vitro. Breast J. 2003 Mar-Apr;9(2):116-9. Central nervous system progression during systemic response to trastuzumab, humanized anti-HER-2/neu antibody, plus paclitaxel in a woman with refractory metastatic breast cancer. Lindrud S, Orlick M, Barnard N, Hait WN, Toppmeyer DL. UMDNJ-Robert Wood Johnson Medical School, Cancer Institute of New Jersey, New Brunswick 08901, USA. Treatment of selected patients with anti-HER-2/neu antibodies alone (1) or in combination with chemotherapy (2) may be of benefit to patients with refractory breast cancer. Approximately 30% of breast cancers overexpress HER-2/neu, a member of the epidermal growth factor receptor family. These patients may have a poorer overall prognosis (3) due to relative resistance to both hormonal therapy and chemotherapy (4-6). We recently observed a patient with refractory breast cancer who responded to rhuMAB HER-2 (trastuzumab) plus paclitaxel after progressing on paclitaxel alone. While on combination treatment she developed cerebellar metastases. Follow-up computed tomography (CT) scan revealed that her disease continued to respond in the liver, lungs, and bone. This case suggests that failure of trastuzumab to cross the blood-brain barrier may compromise its overall effectiveness and raises the possibility that the central nervous system (CNS), or other sanctuary sites, may become clinically more significant in patients with breast cancer in the era of antibody-based therapies. Strahlenther Onkol. 2002 Sep;178(9):486-90. Combined radiochemotherapy with paclitaxel in the treatment of malignant glioma. Schuck A, Muller SB, Kohler A, Konemann S, Wienstroer M, Mosler C, Rube CE, Wassmann H, Willich N, Rube C. Department of Radiotherapy, University Hospital of Munster, Germany. schuck@unimuenster.de BACKGROUND: Paclitaxel is a radiosensitizing agent that shows a synergistic effect with radiation in malignant glioma cells. A phase I/II trial was performed in order to evaluate both feasibility and outcome of combined radiochemotherapy in malignant glioma. PATIENTS AND METHODS: 56 patients were included in the trial. Paclitaxel was administered on days 1-4, 15-18 and 29-32 18 to 24 hours prior to irradiation. Radiotherapy with 60 Gy in conventional fractionation was initiated on day 2.31 patients were included in a dose-escalation trial starting with 20 mg/m2/d and increasing up to 60 mg/m2/d in 10-mg steps. Additional 25 patients were treated with 50 mg/m2/d. RESULTS: The regimen was very well tolerated with minimal subjective impairment such as sickness or weakness. Maximal tolerable dose was 50 mg/m2/d, with neutropenia being the dose-limiting toxicity. There were four allergic reactions and five thromboembolisms; furthermore, one patient with a normal blood count died due to pneumonia. The median survival was 12 months, and significantly favorable factors were a young age, a lower tumor grade (grade 3) and a complete resection. Varying the paclitaxel dose had no influence on outcome. CONCLUSIONS: Combined radiochemotherapy with paclitaxel in the treatment of malignant glioma was well tolerated. Maximal tolerable dose was 50 mg/m2/d. There was no increase in survival compared with results reported in the literature.