Influenza Vaccination
advertisement

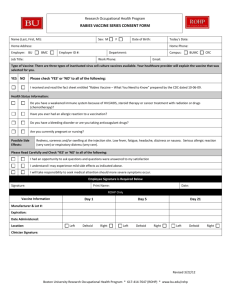
Influenza Vaccination Consent Form 2015/16 Patient ID no (you will find this no. on your repeat medication slip) Patient Details Please complete and Sign Allergies Please circle where appropriate First Name …………………… Surname………………………..Date of Birth ……………………… Age Group: 64yrs and under 65yrs or over Age 2-4yrs Are you allergic to chicken or eggs? Yes / No Do you have any other allergies? Yes / No Patient Signature: …………………………………… Date Vaccine Given: ……………………. ----------------------------------------------------------------------------------------------------------------------- For Completion by Nurse/GP administering the vaccine: For Patients eligible for 2 doses If Yes Please of vaccine pleaseindicate circle to what1………………………… st or 2nd dose. whether 1st Dose 2nd Dose If patient is aged under 65years please indicate below a Clinical Risk/ reason for vaccine Asthma Carer Immuno-suppressed Asplenia COPD Diabetes Liver Disease Chronic Neurological Disease Living in Nursing/Care home Heart Disease Pregnant Kidney Disease Healthcare Worker employed by the Practice --------------------------------------------------------------------------------------------------------------------------------------------------------------------------------- I have explained the procedure to the patient. I have also discussed what the procedure is likely to involve, the benefits and the risks of any alternative treatments (including no treatment) and any other particular concerns of the patient. Given by: ………………………………………………….. Batch No /Expiry Date ………………………. Left / Right Arm No Clinical Risk identified for Flu vaccine Date ………………………. Left / Right Arm