Electrolytes
advertisement

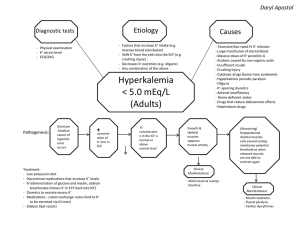
Electrolytes I. The major electrolytes and where they're located A. Intracellular (ICF) vs. Extracellular Fluid (ECF). ICF is the fluid inside cells; ECF is the fluid outside of cells. The two primary compartments of ECF include the interstitium and blood plasma. B. Major ICF electrolytes: K+, Mg+, proteins-, Pi (your book uses HPO4 2-, which is how "free" phosphate typically exists... in any event, what you need to know is "phosphate," and that it's an anion). C. Major ECF electrolytes: Na+, Ca2+ Cl-, proteins- in plasma (there are not many proteins in interstitium but there are lots in plasma). II. Fluid Balance- here, there needs to be a) enough fluid to maintain blood volume/pressure for proper tissue perfusion, b) the proper concentration of solutes (especially Na+) to prevent major fluid shifts from ICF to ECF and vice-versa. This is the primary focus here. A. Dehydration- water loss exceeds water gain. Most commonly caused by excessive perspiration, vomitting, diarrhea. Na+ concentration of the ECF rises: hypernatremia (although typically lots of Na+ is lost during the same types of circumstances). ADH maximizes water retention, urine becomes very concentrate. B. Overhydration- water intoxication. Can be caused by chronic renal failure, endocrine problems (excess ADH), or overconsumption (typically associated with psychological disorders). Na+ concentration of ECF falls, excess water moves into cells, which swell (neuron swelling produces the symptoms) III. Regulating electrolyte concentrations: electrolyte balance. Electrolytes are gained by the diet and lost in a variety of ways: sweat, urine, feces, epithelial sloughing. It is the electrolyte concentration of the ECF that is monitored, and adjustments are made based on that. ECF composition can quickly effect ICF composition throughout the body, because a major part of the ECF travels (plasma). A. Sodium 1. Lost primarily in sweat and urine. 2. Major hormones controlling Na+ loss at the kidneys: a. ADH- when Na+ concentration rises, ADH is released by the posterior pituitary. ADH, as you know, causes water retention. This will cause the concentration of Na+ in the ECF to return to normal (instead of actually getting rid of Na+). b. Aldosterone- when Na+ concentration drops or K+ concentration rises, aldosterone is released by the adrenal cortex. As you know, aldosterone causes Na+ to be reabsorbed and K+ to be secreted via counter-transport. 3. Conditions associated with Na+ imbalances: a. Hypernatremia- A high concentration of Na+ in ECF. Among others, symptoms include a drop in blood pressure and volume, and eventual circulatory collapse. Hypernatremia is caused primarily by dehydration. So the loss of blood volume associated with hypernatremia is connected with dehydration. b. Hyponatremia- Low concentration of Na+ in ECF. Water intoxication: cells swell. Neurons are particularly vulnerable, and symptoms (much like drunkenness) reflect swelling of neurons. B. PotassiumLoss at kidneys is affected by: aldosterone (see above) and simple blood K+ concentration; when it is high, secretion increases and vice versa (simply as a result of more "bumping into" channels that will transport it out). Hyperkalemia (caused by renal failure) and hypokalemia (excess aldosterone or dietary deficiency) both associated with neuromuscular problems, particularly cardiac muscle. C. Calcium- Most calcium is reabsorbed at the kidneys, any excess exceeds transport max and is urinated. However, reabsorption will increase in response to PTH and calcitriol. Hypocalcemia (caused by a dietary deficiency of Ca2+ or vitamin D and hypoparathyroidism) and hypercalcemia (caused by oversupplementation of vitamin D and Ca2+ or hyperparathyroidism) are both associated with neuromuscular problems in addition to other potential symptoms. IV. Acid-Base Balance (Focusing on plasma and acidosis). A. Where do H+ come from? Cellular metabolism. Some common acids: H2CO3 (this is only a buffer if its H+ is taken out of solution and HCO3- is left in solution to pick up OTHER H+) Lactic Acid Ketone bodies Sulfuric and Phosphoric Acids (biproducts of amino acid and nucleic acid breakdown) B. Getting rid of excess H+: Buffers can bind H+ and take them out of solution, but if you keep on producing more (and cells do), pretty soon all the buffers will be saturated and won't be able to bind any more H+. So, in addition to buffers (which temporarily take excess H+ out of solution), we need to be able to get rid of H+ completely. To do this, we can either tie H+ up into a covalent bond in water or we can just excrete the H+. 1. Temporary fixes: buffers. The two most important plasma buffers are proteins and HCO3-. You know how HCO3- is generated and how it works. In addition, cells of the collecting ducts of the kidneys generate HCO3- (guess how!) and simply dump the H+ into the urine. Proteins can also reversibly bind H+. For example, you know that Hb binds H+ in tissues and then lets go of it in the lungs. 2. Permanent Fix #1: Tie H+ up in a covalent bond (respiratory compensation). Remember, in the lungs: HCO3- + H+ --> H2CO3 --> CO2 + H2O. In this way, H+ get stuck into water, and CO2 is removed completely. When cells are very active, lots of CO2 gets produced in tissues (therefore lots of H+, right? what happens in tissues, again?). Respiration increases to rid the blood of excess CO2 (and thereby, excess H+). -Problems with respiratory compensation (not breathing the right amount for the amount of CO2 being produced by cells): Hypoventilation- in this case, you're not getting rid of enough CO2, therefore you are not tying up enough H+ in H2O. Acidosis can result. Hyperventilation- in this case, you're getting rid of too much CO2 and taking too many H+ out of solution. Alkalosis can result. Putting a paper bag over someone's nose when they hyperventilate helps them to recover their CO2 (and therefore H+). 3. Permanent Fix #2: Excrete H+ (renal compensation). When pH drops, the kidneys increase secretion of H+ into urine. (see above, temporary fix, to see where the following fits in) The kidneys also help to regulate blood pH because tubule cells contain carbonic anhydrase. When pH drops, the cells generate HCO3- and H+ (how, again?). The H+ are excreted, and the HCO3- are sent to the blood, in exchange for a Cl-.