DISCLAIMER: As I do not have the answer sheet, don`t simply
advertisement

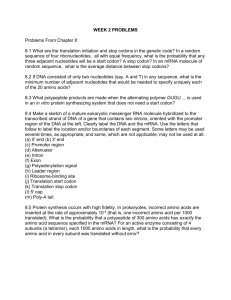
DISCLAIMER: For those of you who thought that tutorial was a waste of time this past week, unfortunately it wasn’t, as we were able to discuss the problem set with Gamal. So I thought I would take the liberty of summarizing what he said for everyone, plus adding my own two cents. As I do not have the answer sheet, don’t simply assume that these answers are correct. And remember, this is just to help you out (a guide), don’t print this out and hand this in, that is still plagiarism. IN TERMS OF REFERENCES, MOST OF THE REFERENCES ARE FROM WIKIPEDIA.COM. 1. Chondroitin is a mucopolysaccharide that is found in the body’s skeletal and soft connective tissue. It has an average molecular weight of ~50 kDa. Based on the biopharmaceutics of absorption for the GI tract, what do you expect the oral bioavailability of this polymer to be (as is and no hydrolyzed)? How likely is a mixture of glucosamine and chondroitin a more efficacious treatment for osteoarthritis than is glucosamine alone? Nonetheless, there have some reports that the addition of chondroitin does indeed produce better results; based on the composition of chondroitin, why might this be? Glucuronic acid Galactosamine Things to consider: Mucopolysaccharide = glycosaminoglycan (GAGs). These molecules are long unbranched polysaccharides containing a repeating disaccharide unit. Chondroitin sulfate is made up of linear repeating units containing D-galactosamine and D-glucuronic acid. The molecular weight of chondroitin sulfate can range from 5,000 to 50,000 daltons (remember, repeating units, it doesn’t specify how many repeating units, but in the question is states that this is the 50000 daltons = 50 kDa) and contains about 15 to 150 basic units (again this one would have 150 basic units) of D-galactosamine and Dglucuronic acid. The oral bioavailability of this drug (as is and not hydrolyzed) would depend on the number of repeating units of the chondroitin. Obviously, since we have the 50000 daltons in this case, the oral bioavailability of unhydrolyzed chondroitin is going to be poor (negligible diffusion, THINK back to medchem and Lipinski's Rule of Five for diffusion: diffusion occurs when molecule is < 500 daltons, has < 5 H-bond donours, has < 5 H-bond acceptor. Obviously these are violated and therefore diffusion is negligable). In addition, there are no active transporters (ie. proteins) for this type of polymer. In addition there are many polysaccharide enzymes (ie. amylase and others) that will break down the polypeptide in the saliva, stomach and intestine, therefore the probability that the intact polymer makes it to the intestine is low. I had a hard time looking up the difference between the efficacy of administering just glucosamine and the combination of glucosamine and chondroitin. Chondroitin may increase joint mobility and slow cartilage loss. In addition, glucosamine is a precursor for glycosaminoglycans, and glycosaminoglycans are a major component of joint cartilage, supplemental glucosamine may help to rebuild cartilage and treat arthritis. So when I was looking up the combination I noticed one thing that the individual dose of glucosamine and the amount of glucosamine in the combination therapy are the same. Therefore, it is highly likely that at the very least, the chondroitin/glucosamine combination should have same efficacy if not more (because the glucosamine at the same strength). If you look at the structure, some of the monomers of chondroitin resemble glucosamine (especially the glucuronic acid subunit). This similarity is structure may allow the chondroitin and glucosamine to be recognized by the same receptor and have similar activity, as a result, a rise in efficacy. 2. Oligodeoxyribonucleotides used as antisense agents are typically much more susceptible to nucleases (which, like proteases, attach unfolded, unprotected substrates) than are aptamers of similar composition. Why? Poon pretty much answered this question in class. To being, recall: polynucleotides such as RNAs and DNAs are formed by the condensation of two or more nucleotides. The condensation most commonly occurs between the alcohol of a 5’-phosphate of one nucleotide and the 3’-hydroxyl of a second, with the elimination of H2O, forming a phosphodiester bond. Furthermore, a nuclease is an enzyme capable of cleaving the phosphodiester bonds between the nucleotide subunits of nucleic acids. Oligodeoxyribonucleotides used as antisense agents are basically SHORT fragments (~12 nucleotides) of DNA that are used to alter the function of target RNAs or DNAs to which they hybridize. Because these fragments are short, they are unable to fold back upon themselves as a resulted their structures are often referred to as “extended” or exposed. In the “extended” conformation, all the phosphodiester bonds are exposed, making it more susceptible to nucleases. Hence the phrase ……fodder for nucleases Moreover, an aptamer, as we saw in the picture at the bottom left hand corner of page 3 of Biologics, tend to be relatively larger (~25 nucleotides) than oligodeoxyribonucleotides. As a result, a single stranded nucleotide (RNA or DNA), using the pairing rules of Watson-Crick (AT, GC), can actually fold back on itself when there are complimentary sequences (see picture at bottom of page 2). The advantage of this folding is that the phosphodiester backbone is tucked in/hidden and therefore the nucleases have a harder time cleaving the phosphodiester bonds, and therefore aptamers are said to be more stable than the oligodeoxyribonucleotides used as antisense agents. 3. Although biologics are generally not bioavailable orally, there are “brute force” exceptions. The structure of desmopressin is shown below. What type of biopolymer is it? What are the intranasal and oral doses of desmopressin? What happens to most of the administered desmopressin when it is given orally? Arrows represent amide bonds (aka peptide bond) You get the picture, there are a lot of them (sorry if I drew an arrow that doesn’t belong or if I missed one). Therefore, this biopolymer is a peptide (oligopeptide). Taken from e-CPS: INTRANASAL: average daily dose for adults is 10 to 40 µg desmopressin and for children 3 months to 12 years of age, 5 to 30 µg. TABLETS: A suitable starting dose for adults and children is 100 µg (0.1 mg desmopressin acetate) three times daily. For patients who have been controlled on intranasal desmopressin and who are to be switched to the oral form, the oral dose producing comparable antidiuresis is about 10-20 times greater than the established intranasal dose. The maximum recommended dosage for both adults and children is 1.2 mg per day (400 µg t.i.d.). Most of the orally administered desmopressin is broken down/cleaved by proteases (digestive enzymes). Proteases are enzymes that break peptide bonds between amino acids of proteins. 4. Why is it impossible/very difficult to produce recombinant antibodies in bacteria? Here are some reasons: - In order for an expressed protein to be active, it has to undergo proper chaperoneassisted folding (which is a post-translational modification). In biology, chaperones are proteins whose function is to assist other proteins in achieving proper folding. In bacteria, however, chaperone assisted folding limited to <100 kDA. Antibodies are big molecules range from 150 kDa and up. Therefore, the protein (antibody) would be folded incorrectly or remain unfolded and therefore be inactive. - bacteria maintains highly reducing conditions. In an active antibody 4 disulfide bridges exist. With this highly reducing conditions, the disulfide bonds do not spontaneously form, rendering the antibody inactive. 5. What is codon bias? Why does a gene construct recovered from a human source sometimes express poorly in a heterologous host? JUST TYPE CODON BIAS IN GOOGLE FOR ALTERNATE DEFINITIONS or CODON USAGE BIAS. Codons are triplets of nucleotides that together specify an amino acid residue in a polypeptide chain. Most organisms use 20 or 21 amino acids to make their polypeptides, which are proteins or protein precursors. Because there are four possible nucleotides, adenine (A), guanine (G), cytosine (C) and thymine (T) in DNA, there are 64 possible triplets to recognize only 20 amino acids plus the STOP signal. Because of this redundancy, most amino acids are coded by more than one triplet. Different organisms often show particular preferences for one of the several codons that encode the same given amino acid. Hence, we have codon bias. Another definition, Codon bias is the probability that a given codon will be used to code for an amino acid over a different codon which codes for the same amino acid. For example, GGT and GGG both code for Glycine but one or the other (usually GGT) is expressed with much greater frequency, hence showing bias. If you look at the top left corner of page 5 (biologics) heterologous hosts include bacteria, yeast, insect cells and mammalian cells. This answer is what I think, and may be wrong, but I think it makes sense (this is prolly the only question I’m not sure about). So different organisms (ie. mammals, insects, bacteria, yeast) express certain genes at different rates because each organism tends to have different priorities. Genes that are always expressed at a high rate should have a different codon bias than those genes that are always expressed at low rates. Therefore, if you take a gene construct from a human source it may sometimes express poorly in a heterologous host because, even though they may code for the same amino acid, the bias is not satisfied. You may put a gene that is expressed low in humans into a heterologous host where that particular gene is expressed at high rates (different biases) and therefore it would express poorly (not favoured).