Document 7652732
advertisement

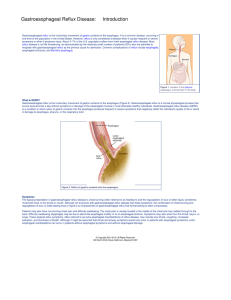
Judy J. Davis, M.D, F.A.A.P. 7405 N. Fresno Street Fresno, CA 93720 (559) 438-8400 Fax (559) 438-1174 Gastroesophageal Reflux in Children Gastroesophageal reflux: (which causes recurrent vomiting or regurgitation) is a common problem and is related to transient relaxations of the lower esophageal sphincter. The lower esophageal sphincter is found between the bottom part of the esophagus and the upper part of the stomach and acts to prevent stomach contents including acid from washing up into the esophagus. When this sphincter does not work properly or when food does not empty out of the stomach normally, vomiting, regurgitation or reflux can occur. In most children the recurrent vomiting is not detrimental to normal growth and development. However, some children develop complications of reflux and they can include irritability, abdominal and chest pain due to irritation of the esophagus from the stomach acid (esophagitis). Poor growth can also develop from reflux due to food being lost through vomiting, or from poor appetite due to pain experienced with reflux (which is usually worse after eating). Reflux may result in anemia due to blood loss from esophagitis. Other complications or reflux include apnea, recurrent pneumonia, bronchitis and asthma from stomach contents washing up into the esophagus and aspirated into the airway (trachea and bronchi), recurrent ear infections, recurrent sinusitis, recurrent sore throat, cavities and hoarseness. A variety of tests can be used in order to diagnose gastroesophageal reflux. These include an x-ray study called a barium swallow or upper GI, which allows the physician to evaluate the anatomy of the esophagus, stomach, and upper intestine to rule out other causes of recurrent vomiting besides reflux. A more sensitive method to rule out reflux is the pH probe which measures the amount of time the esophagus is exposed to an acid environment over a 24 hour period. The pH probe study is sometimes preceded by esophageal manometry which helps locate the lower esophageal sphincter, located between the esophagus and stomach, and also gives some information on how well the esophagus and sphincter perform. Occasionally, a gastric emptying time study is done in order to assess whether the stomach empties more slowly than normal, as well as whether stomach contents are refluxed into the esophagus or if aspiration of stomach contents into the lungs occurs. In most cases, these tests can be done on an outpatient basis. If any of the above studies identify that gastroesophageal reflux is present, endoscopy may be done to rule out esophagitis. Endoscopy allows the physician to look directly at the esophageal tissue and obtain tissue samples for evaluation of esophageal inflammation under the microscope. After gastroesophageal reflux has been diagnosed, medical therapy may be instituted. This could include metoclopramide (Reglan) or urecholine Bethanechol), which tightens the lower esophageal sphincter and improves gastric emptying. Metoclopramide can cause side effects of sleepiness and irritability. Rarely, it causes stiffening of the tongue, back and neck muscles. If stiffening occurs, stop the metoclopramide and take diphenhydramine (Benadryl)____ every six hours for 24 hours. Metoclopramide can also cause movement disorders which may be permanent. These medications should be given 20-30 minutes before feedings to be most effective. Bethanechol should not be given to children with asthma, as it can worsen asthma symptoms. Reglan should not be given to children with seizures, as it can worsen seizure activity. These medications are not as effective in reducing reflux symptoms as the medications that decrease stomach acid production. Agents that stop stomach acid production may be necessary. These include cimetidine (Tagamet), ranitidine (Zantac), famotidine (Pepcid), nizatidine (Axid), omeprazole (Prilosec, Zegerid), rabeprazole (Aciphex), esomeprazole (Nexium), lansoprazole (Prevacid), pantoprazole (Protonix) and dexlansoprazole (Kapidex). Less often, antacids such as Maalox and Mylanta are used. These medicines are used because they increase the healing rate of esophagitis by decreasing the acidity of the stomach contents and prevent the pain that stomach acid causes when it goes up into the esophagus. There are a very small number of children with gastroesophageal reflux who do not respond to medical management. These children may need surgery to tighten the sphincter between the stomach and esophagus to prevent reflux and its complications. The surgery is called a fundoplication. Unfortunately, the surgery doesn’t last forever and reflux will recur in most people. In summary, gastroesophageal reflux is a very common problem in children and 95% of those children are successfully managed with conservative measures and various medications and only a small fraction, approximately, 5% require surgery. If your child does require medical management for his/her gastroesophageal reflux, he/she will be seen in the clinic on a regular basis and monitored for appropriate weight gain and development, evidence of irritability and sleeplessness, pain, anemia and pulmonary problems including apnea, asthma and recurrent pneumonia. Repeating pH probe studies and endoscopy may be necessary to ascertain the effectiveness of medical therapy. If this handout has not answered all of your questions, please call our office at (559)4388400. Judy Davis, MD, FAAP Fellow American Academy of Pediatrics Fellow Sub-Board American Academy of Pediatric Gastroenterology American Board of Nutrition Clinical Professor, Department of Pediatrics, University of California, San Francisco revised 11/09