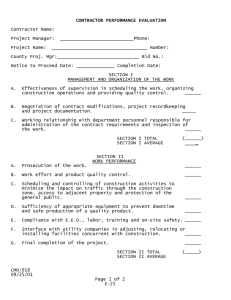
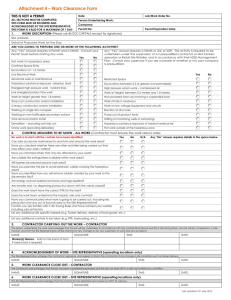
SAFE WORK PERMIT
advertisement

SAFE WORK PERMIT E – Permit Sections 1-5, 8, 12, 13, 16 are required for all jobs (1) BOUNDARY OF WORK (MAINTENANCE/CONTRACTOR) Start Date Start Time Expiration Time (Max = End of worker’s shift) Building Floor Area/Room/Equipment Operating Unit # (Where work is completed) Maintenance Unit/Contractor (Who will perform the work) Phone or Radio # of Maintenance Unit/Contractor (2) HAZARDS OF WORK (MAINTENANCE/CONTRACTOR & OPERATING UNIT) Noise Potential To Be Struck By An Object Heat or Cold Slip or Trip Asbestos Other Hazardous Work/Permits In Area Lead Other: (3) PPE/HAZARD CONTROLS REQUIRED (MAINTENANCE/CONTRACTOR & OPERATING UNIT) Safety Glasses Hard Hat Harness/Retrieval Line (Confined Space) Protective Clothing Type: Goggles(Line Entry) Hearing Protection X-Ray Boundary Chemical Boots Respiratory Protection Type: Face Shield Fall Protection Barricade Area Glove Type: Other Type: (4) WORK DESCRIPTION (MAINTENANCE/CONTRACTOR) Description of Work (How work will be completed - including safety precautions) See Attached None Identified Chemical Flammable or Combustible Product Residue Oxygen Deficiency Dust/Mist/Fumes High Pressure Electrical Elevated Work (>4 feet) Restricted Egress Excavation Mechanical or Pinch Chemicals, Paints, or Solvents Used During JobMSDS’s Must Be Available For All Chemicals NA Specialty Equipment/Tools Used: NA (5) TYPE OF WORK (MAINTENANCE/CONTRACTOR & OPERATING UNIT) Complete Required Sections (1-5, 8, 12, 13, 16) for all jobs. In addition, complete the designated sections for the following types of work: None Of These (Complete Required Sections) Heights>4 ft/Roof/Trestle (Complete Section 6) X-Ray (Complete Section 7) Hot Work (Complete Sections 7, 10) Other Energy Isolation (Complete Section 9) Confined Space Entry (Complete Sections 9-11) Line Entry/Line Break (Complete Sections 9, 15) Demo/Excavation/Crane (Complete KCA Checklists) (6) FALL PROTECTION (MAINTENANCE/CONTRACTOR & OPERATING UNIT) Complete for all Work At Heights Greater Than 4 Feet, Unguarded Roof Work, and Trestle Work Y N Fall Protection equipment/provision required? (“Y” for work on unguarded surfaces >4 ft above adjacent floor OR work outside confines of ladder) Anchor points used? If yes, anchor point is: Engineered Anchor Point I-Beam Structural Steel (7) HOT WORK or X-RAY WORK Complete for all Hot Work or X-Ray Work Other: (MAINTENANCE/CONTRACTOR & OPERATING UNIT) Type I Hot Work - Welding, grinding, burning & open flame cutting Type II Hot Work - Non-rated electrical equipment X-Ray Work Electrical Adapter ID: Inspected prior to use: _______________________ Electrical Adapter ID: Inspected prior to use: _______________________ (Initials) (Initials) Y NA Y NA Y NA Equipment is clean Hot Work signage/X-Ray barrier at work perimeter Area cleared of combustibles (min 35 ft for Type I work) Spark protection/blankets Nearest alarm, phone OR radio identified Fire Extinguisher available at job site (Bring 10 lb. for Type I) Fire or X-Ray Watch assigned (Required for Type I Hot Work OR X-Ray Work only. Must remain at site for 30 min [4 hrs in B-41 truss area] after Hot Work stops) FIRE or X-RAY WATCH INFO Name (Print) Signature Time In Time Out 1st Fire or X-Ray Watch 2nd Fire or X-Ray Watch 3rd Fire or X-Ray Watch 4th Fire or X-Ray Watch (8) PERSONNEL WORKING UNDER PERMIT (MAINTENANCE/CONTRACTOR) I have read this permit and will ensure that its requirements are adhered to. If working conditions change, I will cease work and contact the issuer immediately. I am familiar with emergency procedures for the area where I will be working. I know the location of the closest phone, safety shower, eyewash, and fire extinguisher. Worker Names Organization Contact Info (Phone/Radio#)* I agree with the statements above (initial below) * Contact info required for minimum of one team member Form#: GM00037-E Revised: Jan 09 2009 EMERGENCY PHONE #: 1-2-3 (Cell Phone: 833-4799) SPILL EMERGENCY PHONE #: 3-3800 (833-3800) (9) ENERGY ISOLATION Complete for all Line Entry, Confined Space Entry and Other Energy Isolation (MAINTENANCE/CONTRACTOR & OPERATING UNIT) Y NA Equipment has been properly shut down per appropriate procedure, cleaned, and prepped for energy isolation activities? Existing equipment specific LOTO procedure followed? Procedure # (Energy Isolation Form not required if LOTO procedure is followed) Safe Work Permit Energy Isolation Form followed? Form # (Form not required when isolating single energy sources) All energy sources were verified by each worker that they are isolated properly prior to their work on the system? Includes walking down valves/pumps/etc. Equipment energy isolation has been verified by attempting to start the equipment while in the energy-isolated state. Personal lock applied to Lock Box for group LOTO? (See Section 11 for Confined Space Entry LOTO scenarios). (10) ATMOSPHERIC MONITORING – INITIAL and PERIODIC (MAINTENANCE/CONTRACTOR & OPERATING UNIT) Complete for all Hot Work, or Confined Space Entry All Work: 1. Atmospheric testing personnel (minimum of 2) must be trained in the use of 4. Conduct tests of work area as close as possible to work times. appropriate meters and allow all workers the opportunity to observe tests. 5. Conduct tests in nearby trenches/drains/etc. 2. Both parties must conduct separate BUMP tests, but may use the same meter. 6. When testing work area for flammables, confirm <2.0 % of LEL. 3. Acceptable BUMP ranges are noted in the table below. 7. Re-test required if re-entering space or work area is vacated. Confined Space Entry: 1. Continuous monitoring of Oxygen(O2),Carbon Monoxide(CO),Hydrogen Sulfide(H2S) & Flammables required for sewer entry. 2. Continuous monitoring required if Oxygen levels could be depleted. 3. When testing work area for Oxygen, confirm 19.5% - 23.5% Oxygen in the area. 4. BUMP test and monitor for toxic vapors if potentially toxic atmospheres will be entered.* BUMP Tests Test Results must be within range Operating Unit Maint/Contr. Oxygen Oxygen 18.5% -19.2% Flammable 18.5% -19.2% Flammable 27% - 33% LEL Toxic 27% - 33% LEL Toxic If Applicable* If Applicable* Initial Tests Of Work Area Test 1 Test 2 AREA MONITORING Re-Test 1 Re-Test 2 Re-Test 3 Re-Test 4 Re-Test 5 Time:________ Time:________ Time:________ Time:________ Time:_______ Oxygen-Top CS CS CS CS CS CS CS Oxygen-Bottom CS CS CS CS CS CS CS Flammable-Top CS CS CS CS CS CS CS HW / CS HW / CS HW / CS HW / CS HW / CS HW / CS HW / CS *Toxic-Top CS CS CS CS CS CS CS *Toxic-Bottom CS CS CS CS CS CS CS Operating Unit Maintenance or Contractor Flammable-Bottom Meter ID Name or Initials Unit/Organization * If toxic vapor BUMP test or monitoring is required, list toxic material: _____________ and allowable limit: ____________. Consult EHS for toxic vapor questions. (11) CONFINED SPACE ENTRY (MAINTENANCE/CONTRACTOR & OPERATING UNIT) Complete for all Confined Space Entry ENTRY SUPERVISOR(S) ATTENDANT(S) ENTRANT(S) Name (Print) Name (Print) Name (Print) 1. __________________________________ 1. _____________________________________ 1. __________________________________ Initial to indicate approval to enter: _______ 2. _____________________________________ 2. __________________________________ 3. _____________________________________ 3. __________________________________ 4. _____________________________________ 4. __________________________________ 5. _____________________________________ 5. __________________________________ 3. __________________________________ 6. _____________________________________ 6. __________________________________ Initial to indicate approval to enter: _______ 7. _____________________________________ 7. __________________________________ 2. __________________________________ Initial to indicate approval to enter: _______ Personal Locks (NA if using Energy Isolation Form) Applied Communication between attendant and entrants via: Radio Voice Other:___________ Falcon Horn was tested for functionality: ______(Attendant initials) Radio communication w/Fire Station established & maintained during entry______(Attendant init.) Is forced ventilation required during entry? Yes No (12) ADDITIONAL PRECAUTIONS/INSTRUCTIONS (OPERATING UNIT) Complete if there is a need to describe any Specific Hazards, waste disposal info, and/or other requirements for the work (13) PERMIT APPROVAL (OPERATING UNIT) Y NA Joint walkthrough with operating unit and worker rep required after job Notified other areas of work (Required for Hot Work and X-Ray Work) Unit Representative Name Radio #: _________________ Signature Date/Time (14) UNIT REPRESENTATIVE CHANGE (OPERATING UNIT) If applicable, the outgoing unit representative has communicated the details of this permit/job to an incoming unit representative Incoming Unit Representative Signature Date/Time Radio #: _________________ (MAINTENANCE/CONTRACTOR & OPERATING UNIT) (15) LINE INTEGRITY CHECKLIST NA Complete for all process and service piping after Line Entry is complete and system is being restored Y N Is system returned to a condition allowing pressure testing? If Yes, Maintenance/Contractor may move on to Section 16, and the operating unit will complete the remainder of section 15. If No, finish Section 15 together. Y N NA Y NA Y NA Pressure check will be performed New gaskets used Operating unit positioned valves properly Pressure check not possible-use following precautions Flanges/connections are tight Established and maintained flow/pressure Spill kit is on hand & available Drain/bleed valves are closed Confirmed integrity of system (no leaks) Fugitive Emissions requirements: Operations called 3-6444 for OVA monitoring on tagged equipment. Pressure tests completed on Pressure Test Trains (16) PERMIT COMPLETION (MAINTENANCE/CONTRACTOR & OPERATING UNIT) Maintenance/Contractor To Address The Following Items Prior To Sign-Off Final Sign-off To Close Out This Safe Work Permit Y NA All work relating to this job is completed.(NA = Work will resume later) _________ _ Equipment removed from area (Adapters, Barriers, X-Ray Sources,etc.) Maintenance/Contractor Signature Date Time Notification made to effected workers that work is complete (Required _ ____ after X-Ray work. Must notify Fire Station after Confined Space Entry) Unit Representative Signature Date Time All personal locks are removed from the equipment and/or lock box. Send completed permit to Kalamazoo EHS at PORT-41-16 Form#: GM00037-E Revised: Jan 09 2009 EMERGENCY PHONE #: 1-2-3 (Cell Phone: 833-4799) SPILL EMERGENCY PHONE #: 3-3800 (833-3800)