Depression

DO YOU JUST HAVE THE BLUES?
ARE YOU CLINICALLY DEPRESSED?
The signs of depression are common. We all experience periods of sadness and self- doubt, although these are not usually severe enough to qualify for a psychological diagnosis. Typically, these feelings begin with a reaction to some stressful life circumstance such as losing a job. If these feelings dissipate within 6 months, the American Psychological Association’s DSM-IV labels them as an Adjustment
Disorder with depressive features – a transient reaction to a stressful circumstance.
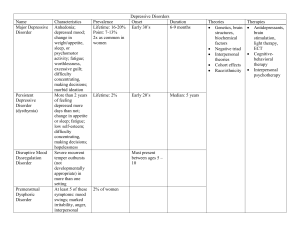
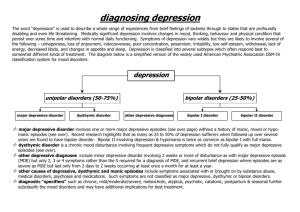
A Major Depressive Episode may appear superficially similar to an adjustment disorder, but it is more extreme. It is not a passing reaction to life’s vicissitudes, but a serious mental disorder. Clinical depression is the “common cold” of psychological disorders. Between 8% and 20% of the population will experience a major depressive episode sometime in their lives (Kessler et al., 1994).
MAIN DSM-IV DIAGNOSTIC CRITERIA FOR A MAJOR DEPRESSIVE EPISODE:
A.
Five (or more) of the following symptoms have been present during the same 2- week period and represent a change from previous functioning at least one of the symptoms is either (1) depressed mood or (2) loss of interest or pleasure.
1.
Depressed mood most of the day, nearly every day as indicated either by a subjective report
(feels sad) or observation made by others. (This may appear as irritability).
2.
Markedly diminished interest or pleasure in all, or almost all activities most of the day, nearly every day.
3.
Significant weight loss when not dieting or weight gain, or a decrease in appetite nearly every day.
4.
Insomnia or hypersomnia (greater than average sleep) every day.
5.
Psychomotor agitation or retardation nearly every day (observable by others).
6.
Fatigue or loss of energy every day.
7.
Feelings of worthlessness or excessive or inappropriate guilt (which may be delusional) not merely self-reproach about being sick.
8.
Diminished ability to think or concentrate or indecisiveness.
9.
Recurrent thoughts of death (not just fear of dying)., recurrent suicidal ideation, or suicide attempt.
B.
The symptoms cause significant distress or impairment in functioning and are not the result of substance abuse or a general medical condition (American
Psychological Association, 1994, p 327).
PSYCHOLOGICAL TREATMENTS: Psychological treatment is designed to help people learn more effective ways of behaving.
Cognitive-Behavioral Therapy combines cognitive and behavioral interventions. The cognitive component involves teaching patients to identify self-critical and negative thoughts, to note the connection between such thoughts and depression, and to challenge negative thoughts to see if they are supportable. If they are not, the patient taught to replace them with more realistic evaluations of present and future circumstances.
Interpersonal Therapy (IPT) aims to help patients examine the ways in which there present social behaviors keep them from forming satisfactory interpersonal relationships. IPT focuses on the present, especially problems in adjusting to grief, fights with friends, co-workers and relatives, role transitions (new job, divorce), and social deficits (such as difficulty in acquiring new relationships). In addition to gaining insight, patients are taught assertiveness and communication skills as well as other ways of improving their ability to form supportive relationships.
Psychoanalytic Therapy is designed to help patients achieve insight and understanding into the repressed conflicts that are presumed to be responsible for their mood disorder. Most often, these conflicts involved the loss of a loved one, accompanied by quilt, the psychologist encourages the person to release and eliminate their inner-directed anger.