Spectral Analysis of Right Hand Ulnar Artery Doppler Signals for the
advertisement

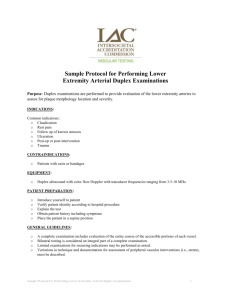
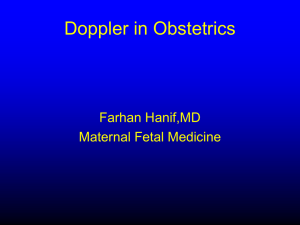
Medical diagnosis of rheumatoid arthritis disease from right and left hand Ulnar artery Doppler signals using adaptive network based fuzzy inference system (ANFIS) and MUSIC method 1 Ali Osman ÖZKAN, 2Sadık KARA, 3Ali SALLI 4 Mehmet Emin SAKARYA and 5Salih GÜNEŞ* 1 Selcuk University, Vocational College of Technical Sciences, 42003, Konya-Turkey 2 Fatih University, Institute of Biomedical Engineering, 34500, Istanbul-Turkey 3 Selcuk University, Meram Faculty of Medicine, Dept. of Physical Med. and Rehabilitation, Konya-Turkey 4 Selcuk University, Meram Faculty of Medicine, Dept. of Radiology, Konya-Turkey 5 Selcuk University, Dept. of Electrical and Electronics Eng., 42035, Konya-Turkey ABSTRACT: Rheumatoid arthritis (RA) is a multi-systemic autoimmune disease that leads to substantial morbidity and mortality. In this paper, as spectral analysis methods of Multiple Signal Classification (MUSIC) method is used in order to extract the significant features from the right and left hand Ulnar artery Doppler signals for the diagnosis of RA disease. The MUSIC method has been used as subspace method. To extract features from Doppler signals obtained from the right and left hand Ulnar arterial the MUSIC method model degrees of 5, 10, 15, 20, and 25 were used. Then, an adaptive network based fuzzy inference system (ANFIS) was applied to features extracted from the right and left hand Ulnar artery Doppler signals for classifying RA disease. In the hybrid model, the combination of MUSIC and ANFIS yielded classification accuracies of 95% (for a model degree of 20) using the right hand Ulnar artery and classification accuracies of 91.25 % (for a model degree of 10) using left hand Ulnar artery Doppler signals in the diagnosis of RA disease. The proposed approach has potential to help with the early diagnosis of RA disease for the specialists who study this subject. Keywords: Rheumatoid arthritis disease; Ulnar artery; MUSIC method; Adaptive network based fuzzy inference system. 1. Introduction 1 Rheumatoid arthritis (RA) is observed in all races worldwide with varying frequency. Genetic factors play an important role and likely account for about 50 % of disease susceptibility [1]. RA is a chronic disease with symmetrical polyarticular involvement and systemic symptoms, such as fatigue and low level fever [2]. RA is an autoimmune disease that causes chronic inflammation in the joints. RA can also cause inflammation of the tissue around the joints, as well as in other organs in the body. Autoimmune diseases are illnesses that occur when the body's tissues are mistakenly attacked by their own immune system [3]. RA is a systemic chronic inflammatory disorder that mainly affects diarthrodial joints. It is characterized by inflammatory activity of synovium leading to the destruction of bone and joint cartilage along with periarticular structures like tendons and ligaments. It is the most common form of inflammatory arthritis and the world prevalence of RA is approximately 0.31.2 % in a female/male ratio of 2.5/1. It is most common in patients aged 40 - 70 years old and its incidence increases with age [4-6]. The Ulnar artery is the main blood vessel of the medial section of the forearm. It arises from the brachial artery and terminates in the superficial palmar arch, which joins with the superficial branch of the radial artery. It is palpable on the anterior and medial section of the wrist [7]. RA disease activity and its therapeutic response is predominantly measured using clinical assessments and laboratory tests for serum markers of inflammation, such as C reactive protein (CRP) or erythrocyte sedimentation rate (ESR). Tenderness and swollen joint counts are essential for physical examinations and evaluating disease activity. They also comprise the Disease Activity Score 28 (DAS 28), which was developed for evaluating disease activity in RA. However, clinical evaluation of joint pain and swelling has not been sufficiently reliable [8]. Direct radiography can be used for evaluating established erosions, but gives us little information on synovial inflammation and early erosions [9]. However, color Doppler ultrasound (CDU) displays blood flow in the tissues and can be a marker of the inflammatory response. Thus, the amount of CDU activity in the inflamed synovium can be used to quantify the inflammatory activity in RA [10]. 2 The Doppler Effect is used in ultrasonic Doppler devices for the measurement and imaging of blood flow transcutaneous. In these devices, ultrasonic waves are launched into a blood vessel by an ultrasonic transducer and the scattered radiation from the moving red cells is detected by either the same or a separate transducer. Appropriate instrumentation is incorporated to extract the Doppler frequency, which is proportional to the red cell velocity [11]. The rebounded echoes are Doppler shifted. The Doppler shift is related to the flow velocity by. f d = f t - fr = 2 υ Cosθ ft c (1) Where f is the mean frequency of the Doppler spectrum, f t is the frequency emitted by the d transducer, f r is the frequency of the returned echo, υ is the flow velocity, θ is the Doppler angle and c is the velocity of sound in blood. For an ultrasound transmitting at frequencies between 1&15 MHz [11], blood flow velocities in the human body generate Doppler-shifted echo frequencies in the audio range. Recent literature compares the Doppler Ultrasound images of healthy subjects and patients having RA disease, and calculates the resistive index (RI) and pulsalite index (PI) of these images [12-16].. Therefore, this study is a novel study using Doppler ultrasound signals on the diagnosis of RA disease. When we look at the studies, it has been observed that doctors have often worked with devices such as Doppler ultrasound and MR images in diagnosing RA disease. Therefore, our study is novel as it is a signal processing from the Ulnar artery Doppler signal. In this study, as spectral analysis method the MUSIC method has been used to extract the significant features from the right and left hand Ulnar artery Doppler signals for diagnosing the RA disease. The detection of RA disease is comprised of three phases: (i) acquisition of the right and left hand Ulnar arterial Doppler signals, (ii) feature extraction using the MUSIC method power spectral density (PSD) graphics obtained from Doppler 3 ultrasound signals taken from the right and left hand Ulnar artery, and (iii) the classification of RA disease as healthy and patient using ANFIS. The MUSIC method model with degrees of 5, 10, 15, 20, and 25 were used in the process of feature extraction from the Doppler signals belonging to the right and left hand Ulnar artery. Later, ANFIS was used to classify the Doppler signals belonging to the right and left hand Ulnar arterial to find out whether the patient had RA or not. ANFIS is hybrid learning algorithms combining the adaptive features of artificial neural networks with fuzzy logic qualitative feature extraction [17-18]. ANFIS uses a hybrid learning algorithm combining the slopped decrease and the least squares method. While the least squares method provides a fast learning, slopped decrease changes membership functions generating the basic functions of the least squares method [17-18]. 2. Material 2.1 Hardware and Demographic Acknowledgments The Ulnar arterial Doppler ultrasound signals were obtained from the right and left hand Ulnar arteries of 40 patients with RA diseases and 40 healthy volunteers. The patients are comprised of 8 males and 32 females, between 38 and 70 years of age, with a mean age and standard deviation of 51 ± 9.6 years. The healthy volunteers are comprised of 10 males and 30 females, between 44 and 73 years of age, with a mean age and standard deviation of 57 ± 9.1 years. The study was approved by the local ethical committee. All subjects gave their written informed consent prior to the study. Doppler signal acquisition was accomplished with a General Electric LOGIQ S6 Power Doppler Ultrasound Unit from the Radiology Department in the Meram Faculty of Medicine of Selcuk University. The system hardware was comprised of a Power Doppler Ultrasound unit that can work in the pulsed mode, a linear ultrasound probe (12 MHz) and a personal computer (Figure 1). A personal computer was used for storing, displaying and performing spectral analysis of the obtained Doppler data. 4 Figure 1. Block diagram of the system hardware used to obtain Doppler data. Before Doppler data was recorded, a color and pulsed Doppler ultrasound examination of the right and left hand Ulnar arterial was performed in order to exclude the presence of a hemodynamically significant stenosis. A linear ultrasound probe of 12 MHz was used to transmit pulsed ultrasound signals into the right and left hand Ulnar arterial. Signals reflected from the arterial were recorded to extract the Doppler shift frequencies. In all tests performed on the patients and healthy subjects, the insonation angle and the presetting of the ultrasound were kept fixing. The insonation angle was adjusted both manually & via electronic steering methods to keep a constant value of 60 degrees on a longitudinal view. The sampling volume was placed within the center of the arterial. The amplification gain was carefully set to obtain a clean spectral output with minimized background noise on the spectral display [19-23]. The audio output of the ultrasound units was sampled at 44.1 kHz and then sent to a computer. Figure 2 shows the Doppler signals for a healthy subject on the right and left hand Ulnar artery, while Figure 3 shows the Doppler signals for a patient having RA disease. Transforming the Doppler signals from the time domain to the frequency domain using the MUSIC method RA disease has been successfully diagnosed. 5 0.5 0 -0.5 -1 0 1 2 3 4 5 Normalized Sound Signal Amplitude Normalized Sound Signal Amplitude 1 1 0.5 0 -0.5 -1 0 1 Time Axis (sec.) (a) 5 2 3 4 Time Axis (sec.) (b) Figure 2. Doppler signals for a subject (no:12) with a healthy (b) left hand Ulnar artery. 1 0.5 0 -0.5 Normalized Sound Signal Amplitude Normalized Sound Signal Amplitude (a) right hand Ulnar artery 1 0.5 0 -0.5 -1 0 1 2 3 4 Time Axis (sec.) (a) 5 -1 0 1 5 2 3 4 Time Axis (sec.) (b) Figure 3. Doppler signals for a patient (no:10) with RA disease on (a) the right hand Ulnar artery (b) the left hand Ulnar artery. The development of quantitative parameters of Doppler flow signals based on spectral analysis has much value in diagnosing arterial disease. Using spectral analysis techniques, the variations in the shape of the Doppler spectra as a function of time are presented in the form 6 of sonograms from which medical information can be extracted [24-25]. A sonogram is plotted with the frequency components and PSD values sequenced on the timeline [26]. The 600 500 450 375 Frequency (Hz) Frequency (Hz) AR sonograms of healthy subjects are shown in Figure 4 and patients in Figure 5. 300 150 250 125 0 0 0 3 1 2 4 Time Axis (sec.) (a) 5 0 1 2 3 4 Time Axis (sec.) (b) 5 Figure 4. AR sonograms developed for a subject (no:12) with a healthy (a) right hand Ulnar artery (b) left hand Ulnar artery. 700 700 525 Frequency (Hz) Frequency (Hz) 525 350 175 350 175 0 0 0 1 3 2 4 Time Axis (sec.) (a) 5 0 1 2 3 4 Time Axis (sec.) (b) 5 Figure 5. AR sonograms developed for a patient (no:10) having RA disease on (a) the right hand Ulnar artery (b) the left hand Ulnar artery. 7 3. Method In this paper, a system with three stages is proposed: the first stage acquires the right and left hand Ulnar arterial Doppler signals; the second stage extracts features using the MUSIC method and the third stage classifies RA diseases using ANFIS based on the right and left hand Ulnar artery Doppler signals. Figure 6 shows the flowchart of the classification systems. The proposed method will be explained in more detail in the following subsections. Measurement of Doppler signals Acquisition of right and left hand Ulnar arterial Doppler signals Feature extraction process Feature extraction from right and left hand Ulnar arterial Doppler signals using the MUSIC method Classification using the ANFIS Classification of right and left hand Ulnar arterial Doppler signals as healthy and RA disease using ANFIS Classification results RA disease or healthy Figure 6. The flowchart of the classification systems. 3.1 Feature Extraction Process of MUSIC Spectral Analysis Method As part of the feature extraction process, the MUSIC spectral analysis method is used to transform Doppler signals from the time domain to the frequency domain. The MUSIC method was proposed by R. O. Schmidt in 1979 as an improvement to Pisarenko's method. It is an algorithm that can be used for frequency estimation [27] and emitter location [28]. The MUSIC method is frequency estimator technique based on eigen-analysis of the autocorrelation matrix. This type of spectral analysis categorizes the information of a correlation or data matrix, as either signal or noise subspace [29]. 8 The MUSIC method estimates the frequency content of a signal or autocorrelation matrix using an eigen-space method. This method assumes that a signal, x ( n ) , consists of p complex exponential in the presence of Gaussian white noise. Given an M M autocorrelation matrix, Rx , if the eigenvalues are sorted in decreasing order, the eigenvectors corresponding to the p largest eigenvalues spanning the signal subspace [27,28]. The frequency estimation function for MUSIC is, P MUSIC (e jW ) 1 2 M H e vi i p 1 (2) T jW 2 jW 3 jW j (M 1)W where vi are the noise eigenvectors and e 1. e .e .e ... e The MUSIC method proposed by Schmidt [30] eliminates the effects of spurious zeros by using the averaged spectra of all the eigenvectors corresponding to the noise subspace [31 - 34]. 3.2 Classification of Right and Left Hand Ulnar Artery Doppler Signals Using ANFIS In this study, we have used ANFIS to classification of right and left hand Ulnar artery Doppler signals. ANFIS was proposed by Jang in 1993 [18]. ANFIS is a class of adaptive networks that are functionally equivalent to fuzzy inference systems (FIS). FIS is the process of formulating the mapping from a given input to an output using fuzzy logic [38]. There are two types of FIS, the Mamdani-type model and the Sugeno-type model. The most frequently investigated ANFIS architecture is the first-order Sugeno-type model, due to its efficiency and transparency [18, 39]. A representative ANFIS architecture with two inputs (x and y) one output (f) and two rules is illustrated in Figure 7, which consists of five layers [39]. 9 Layer 1 Layer 3 Layer 2 A1 M x w1 Layer 4 _ N x Layer 5 y w1 _ w1 f1 A2 S _ B1 y M B2 f w2 N W2 _ f2 W2 x y Figure 7. ANFIS architecture with two inputs one output and two rules. An adaptive system of a fuzzy, first-order Sugeno-type model is considered to facilitate learning and adaptation. Fuzzy if-then rules are [17-18, 40-43]. Rule1: If x is A and y is B then f p x q y r 1 1 1 1 1 1 Rule 2: If x is A and y is B then f p x q y r 2 2 2 2 2 2 (3) In order to apply FIS in ANFIS, two methods including grid partition and subtractive clustering are used. In the process of ANFIS training, we apply subtractive clustering as these partitions the input data according to the dimension of the dataset and automatically tune the input-output membership functions. The least squares method and hybrid learning algorithm are used to identify the optimal values of these parameters, including consequent and premise parameters. We used the hybrid learning algorithm in this process [17-18, 40-43]. 4. Results and Discussion American College of Rheumatology criteria which were used to classify RA diseases in 1987 are still used today [44]. However, early recognition of the disease depends on low originality and sensitivity. These criteria were modified in 1994 [45]. Disease activity and therapeutic response is predominantly based on clinical assessments and laboratory tests for 10 serum markers of inflammation like ESR or CRP. Tender and swollen joint counts are essential for physical examinations and evaluating disease activity [8]. These are the components of DAS 28, which have been developed for evaluating disease activity in RA. Figure 8 shows the location of the 28 joints in our body. Figure 8. Locations of the 28 joints in our body. The DAS 28 values of forty RA patients participating in the study were calculated with the following formula: DAS 28 0,56. TEN 28 0, 28. SW 28 0, 7.ln( ESR) 0, 014.(VAS ) (4) where TEN28 is the tenderness of joint number, SW28 is the swollen of joint number, ESR is the after 1 hour in mm, and PA is the patient’s assessment in mm by a specialist. The average, standard deviation, minimum and maximum values of the DAS 28, VAS, tenderness of joint number, swollen of joint number, ESR and CRP values of forty RA patients participating in the study are given in Table 1. Table 1. DAS 28, VAS, tenderness of joint number, had swollen of joint number, ESR and CRP values of 40 RA patients. Value Mean DAS 28 VAS (mm) Tenderness of joint number Swollen of joint number ESR CRP 4.804 51.5 10 1.3 33.2 20.53 Standard deviation 1.373 19.81 9.526 1.689 18.34 21.16 Maximum value 7.49 80 28 7 75 78.5 Minimum value 2.16 10 1 0 3 3 11 DAS 28 score under 2.6 gives the remission, between 2.6 and 3.2 gives the low disease activity, between 3.2 and 5.1 gives moderate disease activity and also the score of above 5.1 gives the high disease activity. The results related to the disease situation determined according to the DAS 28-values of 40 RA-patients are shown in the Table 2. Table 2. Distribution of patients according to DAS 28 DAS 28 < 2,6 Number of Disease 2 Disease Situation Remission 2,6 < DAS 28 < 3,2 1 low disease activity 3,2 < DAS 28 < 5,1 21 moderate disease activity DAS 28 > 5,1 16 high disease activity Values of DAS 28 Doppler signals reflected from the right and left hand Ulnar artery were recorded to derive out the Doppler shift frequencies as seen in Figure 2 and Figure 3. These signals in the time domain do not contain extra information about existence of the RA diseases. Therefore, these signals were analyzed in the frequency domain to reveal differences between the healthy subjects and patient with RA disease. In this study, as spectral analysis methods the MUSIC method has been used to extract the significant features from the right and left hand Ulnar artery Doppler signals for diagnosing the RA disease. First, the MUSIC method spectral analysis methods were used to extract the relevant features from the Doppler signals belonging to healthy subjects and patients having RA disease. In this part, we have used models of various model degrees (5,10,15,20 and 25) in applying the MUSIC methods to the Doppler signals. For each model degree, the power spectral density (PSD) values were obtained. Then, the PSD values were applied to input of ANFIS to classify the Doppler signals as belonging to either healthy subjects or patients having RA disease. The feature extraction vectors and the classifiers proposed for classification of the right and left Ulnar artery Doppler signals were implemented with the MATLAB software package. In the training and testing of ANFIS, a data partition of 90-10% (72 -8) train-test was 12 used. In our dataset, there are 40 patients with RA diseases and 40 healthy subjects. In totally, 80 subjects were used to test the diagnosis of RA disease. The training input data set consisted of 36 normal and 36 RA patients (72 sets x 129 samples), while the test data set was made of 4 normal and 4 RA patients (8 sets x 129 samples). In order to evaluate the performance of the ANFIS models, we have used three methods: classification accuracy (CA), sensitivity (SEN) and specificity (SPE) analysis, described in the following equations, respectively CA TP TN (%) TP FP TN FN SEN TP (%) TP FN SPE TN (%) TN FP (5) where TP , FP , TN and FN denote true positives, false positives, true negatives and false positives, respectively [29,46]. (1) True positive (TP): a subject with RA disease is detected as a patient diagnosed with RA disease. (2) True negative (TN): a healthy subject is detected as normal. (3) False positive (FP): a healthy subject is detected as a patient diagnosed with RA disease. (4) False negative (FN): a subject with RA disease is detected as normal [29, 46]. In order to evaluate the performance of ANFIS model of the right and left hand Ulnar artery Doppler signals , the classification accuracy, ROC (Receiver Operating Characteristic) curves, sensitivity and specificity values have been used. Table 3 and Table 4 show the obtained ten-fold Cross Validation average test results by ANFIS for classification of the right and left hand Ulnar artery Doppler signals. ROC curves display the relationship between sensitivity (true positive rate) and 1-specificity (false positive rate) across all possible threshold values that define the positivity of a disease [47]. We have given the obtained ROC curves and AUC (Area Under the Curve) values for 5, 10, 15, 20, and 25 in MUSIC method and showed in Figure 9 and Figure 10. 13 Table 3. Obtained ten-fold Cross Validation average test results by ANFIS for classification of right hand Ulnar artery Doppler signals. Model Degree 5 10 MUSIC 15 20 25 Overall average Method CA (%) SEN (%) SPE (%) 91.25 87.5 90 95 88.75 90.5 94.59 87.5 90 95 91.89 91.8 88.37 87.5 90 95 86.05 89.38 Table 4. Obtained ten-fold Cross Validation average test results by ANFIS for classification of left hand Ulnar artery Doppler signals. Model Degree 5 10 MUSIC 15 20 25 Overall average Method CA (%) SEN (%) SPE (%) 87.5 91.25 83.75 85 90 87.5 87.5 90.24 86.49 88.89 90 88.62 87.5 92.31 81.4 81.82 90 86.61 14 Music - 5 Music - 10 Music - 15 Music - 20 Music - 25 AUC 0.913 0.875 0.888 0.95 0.888 Figure 9. ROC curves for model degrees of 5,10,15,20 and 25 of MUSIC spectral analysis method on the early diagnosis of right hand Ulnar artery Doppler signals. Music - 5 Music - 10 Music - 15 Music - 20 Music - 25 AUC 0.875 0.913 0.838 0.85 0.9 Figure 10. ROC curves for model degrees of 5,10,15,20 and 25 of MUSIC spectral analysis method on the early diagnosis of left hand Ulnar artery Doppler signals. 15 5. Conclusion In this paper the MUSIC spectral analysis method have been used to extract the significant features from the right and left hand Ulnar artery Doppler signals for diagnosing the RA disease. RA disease has been diagnosed using an ANFIS classifier with model degrees of 5, 10, 15, 20 and 25 for the MUSIC spectral analysis methods. In this study, we developed an expert diagnostic system for the interpretation of the right and left hand Ulnar artery Doppler signals using MUSIC spectral analysis and ANFIS method. For right hand Ulnar artery, it can be seen in Table 3 that the model degree 20 of the MUSIC method gives the highest degree of classification accuracy (95 %). For left hand Ulnar artery, it can be seen in Table 4 that for a model degree of 10 the MUSIC method gives the highest degree of classification accuracy 91.25 %. The proposed method in this paper is a novel study related to diagnosis of RA disease using right and left hand Ulnar artery Doppler signals belonging to healthy subjects and patients. In the future, we will increase the number of patients and healthy subjects to further vindicate the proposed method. Therefore, this work comprises a preliminary study. This system can help physicians make final decisions for the early diagnosis of RA disease without hesitation. Acknowledgment This work is supported by the Scientific Research Projects of Selcuk University. 16 References [1] Akar S., Akkoç N.,2006. Epidemiology of Rheumatoid Arthritis, Turkıye Klinikleri Journal of Internal Medical Sciences, 2(25);1-6 [2] Hatemi G., Yazıcı H.,2006. Clinical features of rheumatoid arthritis, Turkıye Klinikleri Journal of Internal Medical Sciences, 2(25);12-17 [3] http://www.medicinenet.com/rheumatoid_arthritis/article.htm (last accessed: May, 2010) [4] Lee D. M., Weinblatt M. E. , 2001. Rheumatoid arthritis, The Lancet ; 358: 903-911. [5] Ozgöçmen S. , Özdemir H., Kiris A., Bozgeyik Z. and Ardicoglu O., 2008. Clinical Evaluation and Power Doppler Sonography in Rheumatoid Arthritis: Evidence for Ongoing Synovial Inflammation in Clinical Remission, Southern Medical Journal, 101, 240-245. [6] Carmona L. , Villaverdei V., Garcia C. H., Ballina J. , Gabriel R. and Laffon A.,2002. The prevalence of rheumatoid arthritis in the general population of Spain, Rheumatology 41, 88-95. [7] http://en.wikipedia.org/wiki/Ulnar_artery (last accessed: May, 2010) [8] Naredo E.,Bonilla G.,Gamero F., Uson J., Carmano L. and Laffon A., 2005. Assessment of inflammatory activity in rheumatoid arthritis: a comparative study of clinical evaluation with grey scale and power Doppler ultrasonography, Ann Rheum dis:64, 875-881 [9] Teh J.,Stevens K., Williamson L., Leung J. and Mcnally G., 2003. Power Doppler Ultrasound of Rheumatoid Synovitis: quantification od therapeutic response, The British Journal of Radiology:76, 875-879 [10] Ellegard K., Pedersen S. T., Terslev L., Samsoe B. D., Henriksen M. and Bliddal H., 2009. Ultrasound colour Doppler measurements in a single joint as measure of disease activity in patients with rheumatoid arthritis—assessment of concurrent validity, Rheumatology 48(3), 254-257 17 [11] Shung K. K., 2006. Diagnostic Ultrasound Imaging and Blood Flow Measurements, CRC press, Taylor & Francis Group [12] Kiriş A., Özgöçmen S., Kocakoç E. and Ardıçoğlu Ö., 2006. Power Doppler assessment of overall disease activity in patients with rheumatoid arthritis, Journal of Clinical Ultrasound, vol. 34, No.1, 5 -11 [13] Terslev L., von der Recke P., Torp-Pedersen S., Koeing M. J. and Bliddal H., 2008. Diagnostic sensitivity and specifity of Doppler ultrasound in rheumatoid arthritis, The Journal of Rheumatology 35:1, 49 – 53 [14] Varsamidis K., Varsamidou E., Tjetjis V. and Mayropoulos G., 2005. Doppler sonography in assessing disease activity in rheumatoid arthritis, Ultrasound in Medicine & Biology, vol.31, Issue 6, 739 – 743 [15] Frize M., Herry C., Adéa C., Aleem I. , Karsh J. and Payeur P., 2009. Preliminary Results of Severity of Illness Measures of Rheumatoid Arthritis Using Infrared Imaging, MeMeA 2009 - International Workshop on Medical Measurements and Applications , IEEE ,187 – 192 [16] Strunk J. , Klingenberger P. , Strube K., Bachmann G., Müller-Ladner U. and Kluge A., 2006. Three-dimensional Doppler sonographic vascular imaging in regions with increased MR enhancement in inflamed wrists of patients with rheumatoid arthritis, Joint Bone Spine, 73, 518-522 [17] Jang J-SR., 1992. Self-learning fuzzy controllers based on temporal back propagation. IEEE Transactions on Neural Networks;3(5):714-723 [18] Jang J-S. R.1993. ANFIS: adaptive-network-based fuzzy inference system. IEEE Transactions on Systems Man and Cybernetics ; 23(3):665 – 685 [19] Özkan A. O., Kara S., Sallı A., Sakarya M. E., Gümüş S., Ünal A. and Güneş S. , 2009.The effect of AR model degrees to early detection of rheumatoid arthritis disease, ICCSA 2009, The 3rd International Conference on Complex Systems and Applications,125-129 18 [20] Kara S. and Dirgenali F., 2007, A system to diagnose atherosclerosis via Wavelet transforms, principal component analysis and artificial neural networks, Expert Systems with Applications 32, 632–640. [21] Joseph J. and Brown J. M., 1993. Introduction to Biomedical Equipment Technology, Prentice-Hall,Englewood Cliffs, New Jersey [22] Atikson P., 1982. Doppler ultrasound and its use in clinical measurement, PrenticeHall,Englewood Cliffs, New Jersey [23] Arenson J. W., 1982, Real-time two-dimensional blood flow imaging using a Doppler ultrasound array, McGraw-Hill, NewYork [24] Evans D. H., McDicken W. N., Skidmore R. and Woodcock J. P., 1989. Doppler Ultrasound: Physics, Instrumentation and Clinical Applications, Wiley, Chichester [25] Dirgenali F. and Kara S., 2006. Recognition of early phase of atherosclerosis using principles component analysis and artificial neural networks from carotid artery Doppler signals, Expert Systems with Applications, 31, 643–651 [26] Latifoğlu F., Polat K., Kara S. and Güneş S., 2008. Medical diagnosis of atherosclerosis from Carotid Artery Doppler Signals using principal component analysis (PCA), k-NN based weighting pre-processing and Artificial Immune Recognition System (AIRS), Journal of Biomedical Informatics 41,15–23 [27] Hayes, Monson H., 1996. Statistical Digital Signal Processing and Modeling, John Wiley & Sons, Inc. [28] Schmidt, R.O, March 1986. Multiple Emitter Location and Signal Parameter Estimation, IEEE Trans. Antennas Propagation, Vol. AP-34, 276-280 [29] Marple, S.L.,1987. Digital Spectral Analysis. Englewood Cliffs, NJ: Prentice Hall [30] Swindlehurst, A. L. and Kailath, T., 1993. A performance analysis of subspace-based methods in the presence of model errors, Part II: Multidimensional algorithms. IEEE Trans. Signal Processing. 41:9, 2882–2890 [31] Proakis J.G., Rader C.M., Fuyun L., Chrysostomos L., 1992. Advanced Digital Signal Processing, Macmillan, New York, NY 19 [32] Güler, I., Kara, S., Güler, N. F., and Kıymık, M. K., 1996. Application of autoregressive and fast Fourier transform spectral analysis to tricuspid and mitral valve stenosis. Comput. Methods Programs in Biomed. 49, 29–36 [33] Subasi, A., Erçelebi, E., Alkan, A., and Koklukaya, E., 2004. Comparison of subspacebased methods with AR parametric methods in epileptic seizure detection, Comput. Biol. Med. 36:, 195–208. [34] Porat B., and Friedlander B., 1988. Analysis of the asymptotic relative efficiency of the MUSIC algorithm, IEEE Transactions on Acoustics Speech and Signal Processing. 36, 4532–4544 [35] Wang X. and Paliwal K.K., 2003. Feature extraction and dimensionality reduction algorithms and their applications in vowel recognition. Pattern Recognition, The Journal of The Pattern Recognition Society 36,,2429 – 2439 [36] Welch, P.D. , June 1967,The Use of Fast Fourier Transform for the Estimation of Power Spectra: A Method Based on Time Averaging Over Short, Modified Periodograms, IEEE Trans. Audio Electroacoust. Vol. AU-15, 70-73 [37] Semmlov, J.L., 2004. Biosignal and Biomedical Image Processing, Marcel Deccer Inc. [38] http://www. mathworks.com (last accessed: May, 2010) [39] Sheng S. and Gao R. X., 2006. Optimization of ANFIS with Applications in Machine Defect Severity Classification, 2006 International Joint Conference on Neural Networks, 728 -734 [40] Akdemir B., Kara S., Polat K, Güven A. and Güneş S., 2008. Ensemble adaptive network-based fuzzy inference system with weighted arithmetical mean and application to diagnosis of optic nerve disease from visual-evoked potential signals, Artificial Intelligence in Medicine, 43, 141-149 [41] Sengur A., 2008. An expert system based on linear discriminant analysis and adaptive neuro-fuzzy inference system to diagnosis heart valve diseases, Expert Systems with Applications, 35 , 214–222 20 [42] Buragohain M., Mahanta C., 2008. A novel approach for ANFIS modelling based on full factorial design, Applied Soft Computing, 8 , 609–625 [43] Subasi A.,2007. Application of adaptive neuro-fuzzy inference system for epileptic seizure detection using wavelet feature extraction, Computers in Biology and Medicine, 37 , 227–244 [44] Arnett F. C., Edworthy S. M., Bloch D. A., McShane D. J., Fries J. F., Cooper N. S., et al., 1988. The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis, Arthritis Rheum, 31; 315-324 [45] MacGregor A. J., Bamber S.,Silman A. J., 1994. A comparison of the performance of different methods of disease classification for rheumatoid arthritis. Results of an analysis from a nationwide twin study. J. Rhematol. ; 21;1420-1426 [46] Tarassenko, L., Khan, Y. U., & Holt, M. R. G. , 1998. Identification of interictal spikes in the EEG using neural network analysis. IEE Proceedings—Science, Measurement and Technology , 45, 270–278 [47] Kara, S., Latifoğlu, F., Karahan, Ö. İ. and Kahriman, G., 2007. Spectral Analysis of Portal Vein Doppler Signals Using STFT and AR Modeling in The Cirrhotic Portal Hypertension Patients, Society for Experimental Mechanics, Experimental Techniques,51-56 21 FIGURE CAPTIONS Figure 1. Block diagram of the system hardware used to obtain Doppler data. Figure 2. Doppler signals for a subject (no:12) with a healthy (a) right hand Ulnar artery (b) left hand Ulnar artery. Figure 3. Doppler signals for a patient (no:10) with RA disease on (a) the right hand Ulnar artery (b) the left hand Ulnar artery. Figure 4. AR sonograms developed for a subject (no:12) with a healthy (a) right hand Ulnar artery (b) left hand Ulnar artery. Figure 5. AR sonograms developed for a patient (no:10) having RA disease on (a) the right hand Ulnar artery (b) the left hand Ulnar artery. Figure 6. The flowchart of the classification systems. Figure 7. ANFIS architecture with two inputs one output and two rules. Figure 8. Locations of the 28 joints in our body. Figure 9. ROC curves for model degrees of 5,10,15,20 and 25 of MUSIC spectral analysis method on the early diagnosis of right hand Ulnar artery Doppler signals. Figure 10. ROC curves for model degrees of 5,10,15,20 and 25 of MUSIC spectral analysis method on the early diagnosis of left hand Ulnar artery Doppler signals. TABLE CAPTIONS Table 1. DAS 28, VAS, tenderness of joint number, had swollen of joint number, ESR and CRP values of 40 RA patients. Table 2. Distribution of patients according to DAS 28 Table 3. Obtained ten-fold Cross Validation average test results by ANFIS for classification of right hand Ulnar artery Doppler signals. Table 4. Obtained ten-fold Cross Validation average test results by ANFIS for classification of left hand Ulnar artery Doppler signals. 22