Post Procedure Hepatic Intraarterial Brachy Therapy Physician Orders
advertisement

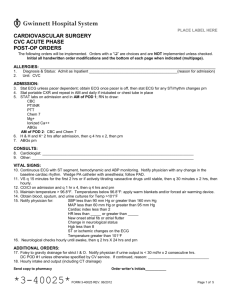
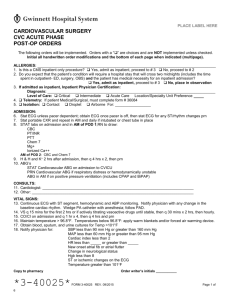
PLACE LABEL HERE POST-PROCEDURE HEPATIC INTRAARTERIAL BRACHY THERAPY PHYSICIAN ORDERS The following orders will be implemented. Orders with a “” are choices and are NOT implemented unless checked. Initial all handwritten order modifications and the bottom of each page when indicated (multipage). Diagnosis Admit as Inpatient: S/P hepatic intraarterial brachy therapy_____________________(reason for admission) & Status: Place in Observation S/P hepatic intraarterial brachy therapy___________________(reason for observation) 1. 2. 3. 4. 5. 6. 7. Unit: _________________________________________ Condition: Fair Other: ___________________________________________________________________ Allergies:___________________________________________________________________________________ Vital signs: see post angiogram orders Activity: see post angiogram orders Diet: Advance as tolerated IVF: ____________________ at __________ ml/hr __________ liters then KVO Medications: 8. Hold medications containing metformin (Glucophage or related medications) for 48 hrs post procedure 9. Antiemetics (choose one): Ondansetron (Zofran) 8 mg IV every 8 hrs prn Promethazine (Phenergan) 12.5 – 25 mg po q 4 hrs prn Other: _____________________________________________________________ 10. Antibiotics: Ceftriaxone (Rocephin) 500 mg IVPB daily or Penicillin AND cephalosporin allergic patients: Cipro 400 mg IVPB q 24 hrs Other: ______________________________________________________________________ 11. Anxiety/restlessness: Ativan 0.5 – 1 mg IV q 4 hrs prn Other: _______________________________________________________________ 12. Severe pain: Hydromorphone (Dilaudid) 0.5 – 2 mg IV q 4 hrs prn Other: ______________________________________________________________________ 13. Moderate pain: Hydrocodone/Acetaminophen (Lortab) 5/500 1-2 tabs po q 4 hrs prn Other: ______________________________________________________________________ 14. Mild pain/temp >100.5°F/HA: Acetaminophen (Tylenol) 650mg po q 4 hrs prn Other: _________________________________________________________ 15. Gastrointestinal prophylaxis: Nexium 40 mg po daily Other: _________________________________________________________ 16. Post-embolization syndrome prophylaxis: Methylprednisolone (Medrol) 40 mg po daily Other: ____________________________________________ 17. Tumor localization scan in nuclear medicine within the first 24 hrs of procedure Additional Orders: ________________________________________________________________________________ _________________________________________________________________________________________________ _________________________________________________________________________________________________ _________________________________________________________________________________________________ _______________ Date ________________ Time _________________________________________ Physician Signature _____________ PID Number Send copy to pharmacy *1-16619* FORM 1-16619 REV. 07/2012 Page 1 of 1 PLACE LABEL HERE POST-PROCEDURE HEPATIC INTRAARTERIAL BRACHY THERAPY PHYSICIAN ORDERS Send copy to pharmacy *1-16619* FORM 1-16619 REV. 07/2012 Page 1 of 1