Patient Consent - BOTOX training
advertisement

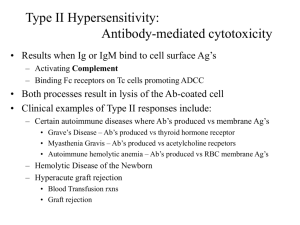
Patient Consent Form-Example Dermal Fillers: Hydrafill/Juvederm/Restylane/Perlane/Laresse Botox-Vistabel Patient Name: ________________________________________ Date of Birth: _____________ I have read the information provided by K-T Training regarding the procedure I will be undertaking. I understand the information given and any questions or queries I have had have been answered. Any medical terminology used in this consent has been explained to me. I am aware of all the risks that are associated with the procedure I will be undertaking. Botox-Vistabel® I am aware that Vistabel® is the trade name for botulinum toxin and it will produce muscle weakness and paralysis. I understand that it may take 1-2 days to start working and the maximum effects may not be reached until 21 days post treatment. I am also aware that repeat treatments may be required every 3 months. The following possible side effects have been explained to me. Bruising, swelling, bleeding, infection at the injection site, drooping of eyelids and eyebrow, double vision, headaches, itching allergic reaction, weakening of untreated muscles, development of antibodies to subsequent treatments. I do not have any of the following contraindications such as Neuromuscular disorders i.e. Myasthenia Gravis or Lambert-Eaton syndrome, dysphasia (swallowing difficulties), Chronic respiratory hypersensitivity to any ingredients to be injected, pregnant or breast feeding. I confirm that I am not taking any of the following medications: aminoglycoside antibiotics, spectinomycin, anticoagulants, aspirin, muscle relaxants or recent anaesthetics. Hydrafill-Juvederm/Restylane/Perlane/Laresse I am aware that Hydrafill, Juvederm, Restylane, and Perlane are non-animal hyaluronic acid and designed to fill facial lines for facial contouring and lip augmentation. I understand that more than one treatment session may be required to obtain maximum effects. The possible side effects have been explained to me and may include redness, swelling, bleeding, bruising, pain, itching, infection, discoloration and hypersensitivity. I am aware of the following contraindications-post allergic reaction or hypersensitivity to the product. I am aware that I am acting as model for the Advanced Botox and Dermal Filler procedure and I am aware that the individuals who are administering the procedure are being trained and are supervised by an experienced trainer. Patient Signature______________________________ Date: _____________