Lecture thirteen--------------------------------------------------------------crown and bridge
احمد غانم.د
Dental porcelain
The term ceramic is defined as any product made essentially from a
nonmetallic material by firing at a high temperature to achieve desirable
properties. The term porcelain refers to a family of ceramic materials
composed essentially of kaolin, quartz, and feldspar, also fired at high
temperature. Dental ceramics for ceramic-metal restorations belong to
this family and are commonly referred to as dental porcelains.
The laboratory portion of a ceramic restoration is usually made in a
commercial dental laboratory by a skilled technician working with
specialized equipment to the shape and shade specifications provided by
the dentist. Skilled technicians and artisans are also employed by the
manufacturers of artificial denture teeth to produce the many forms,
types, and shades necessary in this application of porcelain. Dental
ceramics were first used in dentistry in the late 1700s.
Porcelain jacket crowns were developed in the early 1900s. They
consisted of feldspathic or aluminous porcelain baked on a thin platinum
foil and can be considered the ancestors of all-ceramic crowns. Because
their low strength, however, porcelain jacket crowns were limited to
anterior teeth. In the 1960s, the poor match in thermal expansion (and
contraction) between framework alloys and veneering ceramics, which
often led to failures and fractures upon cooling, stimulated the
development of leucite-containing feldspathic porcelains. The problem
was solved by mixing controlled amounts of high-expansion leucite with
feldspar glass at the manufacturing stage. This allowed the adjustment of
the coefficient of thermal expansion of feldspathic porcelains to very
narrow specifications. This invention led to considerable improvement in
the reliability of ceramic-metals and allowed ceramic materials to be
1
Lecture thirteen--------------------------------------------------------------crown and bridge
bonded to a metal framework. During cooling, the thermal contraction of
the metal framework is slightly higher than that of the veneering ceramic,
thus placing the internal surface of the ceramic in compression. Because
ceramics are stronger in compression than in tension, this property is used
to advantage to provide increased resistance to shattering.
Classification of dental ceramics:
Dental porcelains are classified into four groups:
1. High fusing porcelain (1300-1370 ºC).
2. Medium fusing (1100-1250 ºC).
3. Low fusing (850-1100 ºC).
4. Ultra low fusing < 850ºC.
The high and medium fusing porcelain are used for denture teeth, while
the low and ultra low fusing is used for crown and bridge construction.
Composition:
1. Feldspar.
2. Quartz.
3. Kaolin.
4. Pigments and flux.
1. Feldspar:
It’s the main component of the porcelain about 80% by weight. It’s a
mixture of potassium alumino silicate (K2O.AL2O3.6SIO2) and sodium
alumino silicate (Na2O.Al2O3.6SiO2). The feldspar fused when it melts
forming translucent glass matrix.
2
Lecture thirteen--------------------------------------------------------------crown and bridge
2. Quartz:
It forms about 15%, it acts as strengthening agent and present as fine
crystalline dispersion throughout the glossy phase that is produced by the
melting of the feldspar.
3. Kaolin:
It’s about 4%, it’s a hydrated aluminum silicate (Al2O.2SiO2.2H2O) act as
a binder and increasing the ability to mold the unfired porcelain and aid
in forming a workable mass of porcelain during molding, it’s opaque in
color.
4. Pigments and flux:
It represents less than 1%; some coloring pigments (metallic oxide) are
added in small quantities to provide wide variety of colors, e.g. iron oxide
(brown shade), titanium oxide (yellow shade), and cobalt oxide (blue
shade).
Fluxes (low fusing glass) added to reduce the temperature that is required
to set the porcelain powder particles at low temperature enough, so that
the alloy to which it is fired, do not melt or get deform.
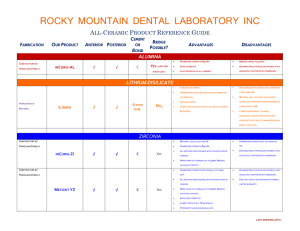
APPLICATIONS:
Ceramics have three major applications in dentistry:
(1) ceramics for metal crowns and fixed partial dentures.
(2) all-ceramic crowns, inlays, onlays, and veneers, when esthetics is a
priority,
(3) ceramic denture teeth.
3
Lecture thirteen--------------------------------------------------------------crown and bridge
Bonding between ceramic to metal.:
1. Mechanical bond:
By mechanical interlocking of porcelain with the roughness of metal
coping (sandblasting the metal surface with aluminum oxide particles).
2. Vander Wall’s bonding:
It’s the attraction between the atoms or molecules, it is adhesion related
to the extent to which the metal is melted by the porcelain, the better
wetting, the stronger the Vander Wall’s adhesion (bond).
3. Compression (physical bond):
The coefficient of thermal expansion for the metal should be slightly
higher than that of porcelain, so that the porcelain will draw toward the
metal when the restoration cools after firing.
4. Chemical bonding:
Metal and porcelain reacts chemically in an oxidized atmosphere at
approximately 1000ºC to bond together (indicated by the formation of an
oxide layer on the metal). The fused porcelain absorbs ions from the
metal to produce a chemical bond between them.
*** 20% of the bond is due to the first three factors, and 80% of the bond
is due to chemical bond.
Porcelain is built in three layers:
1. Opaque layer: it is the first layer applied on the metal to mask the
color of the metal and it is responsible for the metal ceramic bond.
2. Dentine layer.
3. Incisal layer: this is translucent and affected by the color of the
dentine layer.
4
Lecture thirteen--------------------------------------------------------------crown and bridge
The powder is mixed with water and binder (which will help to held the
particles together) and applied to the die either by spatulation, rush
application, whipping or vibrating. The objectives of these techniques are
to remove as much water as possible resulting in a more compact
arrangement with a high density of particles which minimize the firing
shrinkage.
The thermal contraction of porcelain will be resisted by the metal and a
compressive stress will be setup in the porcelain and will be firmly
bonded to the metal.
Properties of porcelain:
1. Esthetic: it has better look than acrylic (looks like vital tooth).
2. Color stability: glazed porcelain will provide a smooth surface
which not allow adherence of stains, while the color of acrylic
facing will change with time due to the porosity and rough surface
of acrylic material.
3. Dimensional stability: the thermal coefficient and conductivity is
close to that of the tooth structure that is why the microleakage is
less likely to be a problem in the presence of good marginal seal,
while in acrylic there is more microleakage because of the higher
coefficient of thermal expansion than that of the teeth.
4. Irritation of the soft tissue: glazed porcelain close to gingival tissue
will not cause inflammation because it’s very smooth which
prevent plaque accumulation while the acrylic will cause gingival
inflammation due to its porosity.
5. Bonding: the bonding between the porcelain and the metal is strong
because it’s (mechanical, physical and chemical in nature)while the
acrylic is mechanically bonded to the metal (by creating a rough
surface with loops and beads).
5
Lecture thirteen--------------------------------------------------------------crown and bridge
6. Abrasion and wear resistance: glazed porcelain has high resistance
to abrasion, while the acrylic facing will be abraded with time. The
compressive strength of dental porcelain is high (350-550 MPa)
while tensile strength is low (20-60 MPa) so the porcelain is hard
but brittle.
7. Staining and glazing: stain can be applied to porcelain which can
be glazed to give highly smooth surface.
6
 0
0