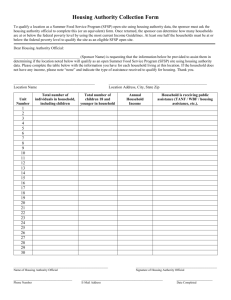
total in household/children & adults_______total
advertisement

THE SALVATION ARMY – CAMP SEBAGO TO BE COMPLETED BY PARENT/GUARDIAN - Please Print Name of Camper Corps or Unit______________________________________ Birth Date Age Boy Girl____________ Zip____________ Home Address City State Parent Phone Work________________________ Address City State Zip_____________ Emergency Phone ________________________Relationship to Camper____________________________________________________________ Section 9(d) of the National School Lunch Act requires that, unless the participant’s Food Stamp, or TANF number is provided, you must include the social security number of the household member signing the statement or an indication that the household member signing the statement does not possess a social security number. Provision of a social security number is not mandatory, but if a social security number is not provided or an indication is not made that the adult household member signing the statement does not have one, the statement cannot be approved. The social security number may be used to identify the household member in carrying out efforts to verify the correctness of information reported on this application. These verification efforts may be carried out through program reviews, audits, investigations, and may include contacting employers to determine income, contacting a food stamp, or TANF office to determine current certification for receipt of food stamps, or TANF benefits, contacting the state employment security office to determine the amount of benefits received, and checking the documentation produced by the household member to prove the amount of income received. These efforts may result in a loss or reduction of benefits, administrative claims, or legal actions if incorrect information is reported. Summer Food Program Eligibility Statement - The Salvation Army Camp Sebago serves nutritious free meals as part of the federally funded Summer Food Service Program for Children (SFSP). Children are defined by the SFSP as being 18 years of age and under or persons over 18 who are determined by a state or local public educational agency to be mentally or physically disabled. In order to be eligible for the SFSP, we must document the number of enrolled children with household incomes less than or equal to the SFSP family size/income guidelines. With your cooperation, we can qualify for federal reimbursement and keep costs to you at a minimum. Please complete and sign the back of this form. Racial/Ethnic Category: Please check the racial or ethnic identity of your child. You are not required to answer this question. This information is being collected to be sure that everyone receives benefits on a fair basis. No child will be discriminated against because of race, color, national origin, sex, age or disability. _____White, not of Hispanic origin _____Black, not of Hispanic Origin _____ Hispanic _____ Asian or _____American Indian or Pacific Islander Alaskan Native Non-Discrimination: This facility is operated in accordance with USDA policy which does not permit discrimination because of race, color, national origin, sex, age or disability. Any person who believes that he or she has been discriminated against in any USDA related activity should write immediately to the Secretary of Agriculture, Washington D.C. 20250 2008 SFSP FAMILY SIZE/INCOME GUIDELINES Households with income less than or equal to these rates are eligible for free meal benefits. Household Size 1 2 3 4 5 6 7 8 Month $1.107 1,484 1,861 2,238 2,615 2,992 3,369 3,746 For each additional family member add: $377 REVERSE SIDE OF FORM MUST BE COMPLETED 2008 MAINE SUMMER FOOD SERVICE PROGRAM - INCOME ELIGIBILITY APPLICATION PLEASE PRINT - COMPLETE EITHER PART 1 OR PART 2 - AND SIGN FORM. Part 1 - For Children receiving Food Stamps or TANF benefits ┌────┐ └────┘ Yes, I received Food Stamps or TANF this month for the child listed on the front of this form, and request meal benefits. Food Stamp Number TANF Number______________________Foster Child Monthly Income________________ Part 2 - For Children not receiving Food Stamps or TANF HOUSEHOLD MEMBERS AND MONTHLY INCOME: List the names of everyone living in your household including yourself, all related and nonrelated individuals, and children. List all income received last month on the same line with the person who received it. List each amount under the correct title. You must list gross income BEFORE deductions, taxes, or social security, etc. To figure monthly income, if income is received: every week, multiply the total gross income x 4.33; every two weeks, multiply the total gross income x 2.15; twice a month, multiply the total gross income x 2. HOUSEHOLD MEMBERS INCOME BY SOURCE LIST ALL OTHER MEMBERS' NAMES (Last, First) MONTHLY EARNINGS FROM WORK BEFORE DEDUCTIONS MONTHLY WELFARE, CHILD SUPPORT, ALIMONY MONTHLY PENSIONS RETIREMENT, SOCIAL SECURITY ALL OTHER MONTHLY INCOME 1. 2. 3. 4. 5. 6. TOTAL IN HOUSEHOLD/CHILDREN & ADULTS_______TOTAL HOUSEHOLD MONTHLY INCOME $__________ PENALTIES FOR MISREPRESENTATION: I certify that all of the information included on this application is true and correct. If Part 1 is completed, the food stamp and TANF numbers are correctly reported, or, if Part 2 is completed, that all income is reported. I understand that this information is being given for receipt of federal funds; that program officials may verify the information on this application; and that deliberate misrepresentation of the information may subject me to prosecution under applicable state and federal laws. The person herein described has permission to engage in all prescribed camp activities, except as noted by the examining physician stated on the Health and Examination Form. Emergency Authorization: I hereby give permission to the medical personnel selected by the camp director to order X-rays, routine tests, and treatment for my child in the event I cannot be reached in an emergency. I hereby give permission to the physician/nurse selected by the camp director to hospitalize, secure proper treatment for, and order injection and/or anesthesia and/or surgery for my child as named above. This form may be photocopied for use out of camp. With respect to photographs taken during my child’s attendance at Camp Sebago, I relinquish all legal rights for payment or redress in their use in public or private circulation. With respect to camp phone usage, it is understood that the Camp Office Phone will be used only by campers in an emergency (under the jurisdiction of the camp director). A pay phone will be made available to campers during specifically outlined times and with the provision of a phone card by the parent or guardian. X _______________________ Address ______________ Signature of Parent/Guardian (required) Social Security Number _____________________ Zip Code _____APPROVED Daytime Phone _____DENIED Date