MEMBERSHIP APPLICATION
advertisement

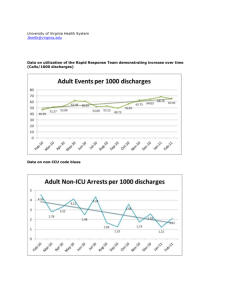
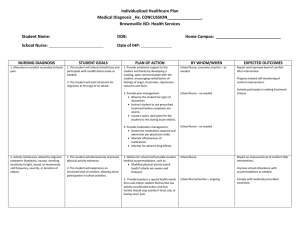
Ocean County School Nurses Association MEMBERSHIP APPLICATION Name:_________________________________________________________________ Home Address:__________________________________________________________ City:___________________________________________ Zip Code:_______________ Home/Cell Telephone Number: ( )______________________________________ Email Address:__________________________________________________________ School:________________________________________________________________ School Address:_________________________________________________________ City:___________________________________________ Zip Code:_______________ School Telephone Number ( )__________________________Ext.:____________ School Email Address: ___________________________________________________ School Fax_____________________________________________________________ □ □ Renewal New Member PLEASE CHECK ONE OF THE FOLLOWING REGULAR MEMBER: Currently full time certified school nurse or supervisor employed by a public Board of Education in Ocean County…………………………………………………………………………………….$20.00 ASSOCIATE MEMBER: Non-certified school nurse, non-working school nurse enrolled in a certification program, substitute school nurse, school nurse employed by a Board of Education outside Ocean County or by a non-public school……………………………………………….$15.00 RETIRED MEMBER…………………………………………………………………………………$10.00 PLEASE SEND THIS COMPLETED FORM AND CHECK BY JUNE 30TH TO: School Nurse Marella-OCSNA North Dover Elementary 1759 New Hampshire Ave. Toms River NJ 08755 MAKE CHECKS PAYABLE TO OCSNA, NO PURCHASE ORDERS OR VOUCHERS ACCEPTED! I am a member of the NJ State School Nurses Association for _______years. I am a member of the National Association of School Nurses for ______years. I am interested in helping on a committee_____________________________