Annual Report 2013-2014
advertisement

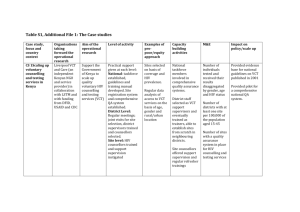
Aastha Friends Affected & Infected Together in Hand (FAITH) ANNUAL REPORT FY 2070-2071 (2013-2014) P.O.Box: 546 Museum Marg, Chhauni-13 Email: faith@faith.org.np Table of contents: 1. EXECUTIVE SUMMARY……………………………………………………………………………..................3 2. ORGANIZATIONALINTRODUCTION.…………….…………………………………………………............4 3. PROGRAMS DETAILS.…..……………………………………………………………………………………........5 3.1National Tuberculosis Programme (NTP) ……………………………………………..…………..........5 3.2. Nepal Round 10 Proposal to Contribute to the Achievement of MDGs 4, 5, 6…………..7 3.3. Intensified early and increased TB case detection amongst children (0-14 years) ….….9 4. MAJOR ACCOMPLISHMENTS..…………………………………………………………………….................12 5. SUMMARY OF FINANCIAL DETAILS..……………………….………………………………………………...12 2 1. EXECUTIVE SUMMARY FAITH’s annual report provide details of the progress made on the core organizational strategy and action plan to achieve its goal to support in national HIV and TB response in Nepal. This report also describes the vision, policy and strategy of FAITH. This annual report covers Shrawan 2070 to Asar 2071 (mid July 2013 to mid July 2014) period. Under the ‘National Tuberculosis Programme (NTP), Nepal Support Project’, FAITH implemented GFATM National Strategy Application (NSA) Phase 2 year 1 program as the Sub-recipient from 13th February 201 3 – 15th July 2014. FAITH conducted the NTP program in Far Western region of Nepal – mainly in Kailali, Baitadi, Achham, Doti, Kanchanpur and Dadeldhura. Through this program, FAITH contributed in health system strengthening by enhancing capacity of human resources from government and non- government on VCT, basic TB/HIV co-infection, basic TB as per the national guideline. The activities included trainings, orientation, sensitization, workshops, advocacy campaign along with awareness activities in colleges and institute of health sciences. Moreover, meetings were held to establish linkage (feedback, referral etc) between DOTS and VCT centers, DOTS and private health practitioners and so on. Furniture and other necessary support were also provided with the objective to strengthen the service delivery sites in concerned districts. Situation Analysis of TB/HIV collaboration and mapping of service providers in Dadeldhura district was also conducted. With support from Save the Children, Nepal, FAITH implemented the Comprehensive HIV and AIDS program and facilitate the delivery of services to the People who Inject Drug (IDUs) in Kanchanpur district. FAITH reached PWIDs through BCC activities and identified and enrolled 157 new IDUs in the Harm Reduction program. In this project, activities to create enable environment like Stigma and Discrimination reduction through orientation to Police Personnel, interaction meeting with Media Personnel, Days Observation (AIDS, Condom, Candle Light and Drug Day), orientation to Community Member/ Clubs and orientation to Family Members were implemented. IDUs related message broadcasted through local FM. Condom promotion and distribution was done. IEC were distributed through DIC centres and outreach workers. The IDUs were referred for VCT, ARV, PMTCT, TB, CHBC, Hepatitis Diagnosed and Treatment Services and Detox and Drug Treatment with emphasis to women drug users. FAITH successfully implemented the project “Intensified early and increased TB case detection amongst children (0-14 years)” to detect additional TB cases among children with support from A Stop Tb Partnership – WHO, TBREACH. The project was implemented in following ten districts - Kavre, Kathmandu, Chitwan, Makwanpur, Parsa, Bara, Rautahat, Sarlahi Mahottari and Dhanusa. The project time period is from 15th February 2013 – 15th July 2014. The primary target population of the proposed project was children (0-14) who were in immediate contact of TB positive, Children Affected by AIDS (CABA) and whose parents were living with HIV. The project targeted to screen 27052 children from the 10 project districts and identify 790 childhood TB cases in its project duration. The project achieved to screen 28513 children out of which 59 SS+ and 394 all forms cases were identified and enrol in DOTS centre. 3 2. ORGANIZATIONAL INTRODUCTION: FAITH is a non-profit making organization established in the year 2005, run by and for the marginalized groups such as people living with and affected by HIV and AIDS, people who use drugs and sexual minorities. It advocates for issues through various channels of mass media mobilization. Mission Statement: To ensure the fundamental rights of people especially women and children from disadvantaged, marginalized and vulnerable groups to live a free and dignified life. Objectives: To advocate for the greater and meaningful participation of disadvantaged, marginalized and vulnerable groups in policy and decision-making. To support for effective and efficient health services delivery. To increase and sustain socio-economic development of the disadvantaged, marginalized and vulnerable groups. Target Population: People especially women and children from disadvantaged, marginalized and vulnerable groups focusing on: People Living with HIV and AIDS Injecting Drug Users Commercial Sex Workers Mobile Population and Sexual Minorities Methodology: Social and economic reintegration Participatory approach Livelihood programs Fund raising Working areas: Organize awareness, sensitization workshops, trainings, and national level interaction and advocacy programs. Conduct research on specific issues. Design and implement awareness and advocacy programs through various modes of communication like radio, television, online media and print media. Develop information, Education and communication (IEC) materials Developing audio/visual documentaries, Public Social Announcement (PSA), music videos and movies incorporating advocacy and social messages. Design and develop innovative program module for strengthening of community-based organization. Organize fund raising events. 4 3. PROJECT DETAILS: 3.1. National Tuberculosis Programme (NTP): Under the ‘National Tuberculosis Programme (NTP), Nepal Support Project’, FAITH implemented GFATM National Strategy Application (NSA) Phase 2 year 1 program as the Sub-recipient from 13th February 2013 – 15th July 2014. The project implementing partners were Naya Goreto (NG) and National Federation of Women Living with HIV/AIDS (NFWLHA). FAITH chiefly contributed in the National Tuberculosis program by implementing all SDAs in Far western region especially Kailali, Baitadi, Achham, Doti, Kanchanpur and Dadeldhura. The Service Delivery Areas (SDA) including: Improving diagnosis High quality DOTS, Practical approach to Lung Health (PAL) TB/HIV collaboration (TB/HIV); All care providers (PPM / ISTC - Public-Public, Public-Private Mix (PPM) approaches and International standards for TB care), Advocacy, communication, and social mobilisation (ACSM). Major activities: SDA: Improving Diagnosis 3.1.1.12: Basic Modular Training for Z-N microscopy (GoN) SDA: PAL 4.1.1.8: Conduct Training for District supervisors, HA and SNs and other BHS) 4.1.1.10: Conduct PAL training Basic Health Staff (Hospitals, PHC, HP and SHP with collaboration of medical collages, Regional and Zonal hospitals. 4.1.1.12: Conduct PAL training for upgraded as AHW and ANM (HP and SHP) SDA: TB/HIV Collaboration 5.1.13: Equipments (Computers, software, printers for PR and SR) 5.3.3: Conduct VCT training for health workers working in TB treatment centre - public and private sector 5.3.5: Basic TB/HIV training to BHS staff (DOTS and VCT centre) and NGOs 5.3.7: TB/HIV training to PLHIV group through their existing network in TBHIV implementing district 5.3.9: Treatment literacy and treatment adherence training to TB/HIV co-infected 5.3.10: Basic TB training for health workers working in HIV/AIDS (public NGOs, private sector) 5.3.11: TB/HIV orientation to volunteers and support groups 5.4.3: Situational analysis (district level) to identify stakeholders for TB/HIV collaboration and map service providers 5.4.6: Strengthen referral system between VCT and DOTS, and/or integration of VCT/DOTS in existing centers 5.5.1: Workshop to establish and scale- up cross referral system between VCT and DOTS centres /sites 5.5.2: Establish DOTS centre in certain VCT/ART sites 5.5.3: Carry out intensified TB case finding among HIV vulnerable groups 5.5.8: Carry out intensified HIV case finding amongst all TB patients in target district at registration 5 5.5.8.1: Health product materials for Carry out HIV testing (Rapid test kit) of all TB Cases in HIV implemented districts 5.5.8.2: Incentive for Carry out HIV testing (Rapid test kit) of all TB Cases in HIV implemented districts 5.6.2: TB/HIV advocacy campaign for NGOs/CBOs working in HIV 5.6.8: TB/HIV sensitization to District AIDS coordination committee, TB/HIV coordination subcommittee, District Development committee members 5.6.9: TB/HIV orientation to village development committee members, DOTS committee 5.9.1: Training for health workers regarding R&R system SDA: PPM 7.2.3: Establish and strengthen TB service delivery centers/sub centers in line with PPM/ISTC (e.g. factories, slum areas, prisons, health institutions including private and public) 7.2.4: Establish linkage (referral, feedback, etc) between existing DOTS centers and private health care providers 7.3.4: PPM/ISTC orientation at Institute of Health Sciences providing education to Paramedical, Nurse, Community Health Worker etc. 7.3.24.2: Strengthen PPM through municipality/ Support 75.3: Private Health Care Providers (Pharmacist, private lab, medical shops, paramedical and other health care providers) reporting four monthly meeting SDA: ACSM 8.2.4: Develop capacity of school health teachers on TB education in districts 8.2.12: Identify cured TB patient and develop their capacity to motivate other TB patients and their families to continue TB treatment 8.3.9: TB awareness activities among Urban Colleges (Urban areas) Major outcomes: Capacity development of 321 human resources from government and non- government following per the national guideline – out of which 15 - lab, 201 - PAL, 105 – TB/HIV component. More than 1000 people including general, people working in TB and HIV as well as TB patients and those belonging to the MARPs group are informed about TB-HIV coinfection through school health program, sensitization meetings and testing campaigns. A situation analysis of TB/HIV collaboration and mapping of service providers was done successfully in Dadeldhura district. 374 HIV vulnerable groups were screened for TB and 29 TB patients were tested for HIV. Issues/challenges Limited time for implementation (activities need to be completed within 5 months). Due to monsoon season and peak of activities to accomplish by the end of fiscal year of the government officials, it was a difficult implementation period. Frequent changes in the work plan and budget that created some challenges in coordination with the DHO and DTLOs. It was difficult to motivate TB patients for HIV testing due to stigma associated with it. 6 Limited TB affected groups focused program/activities which could lead to ensure their active involvement in TB case findings and treatment outcomes. 3.2. Nepal Round 10 Proposal to Contribute to the Achievement of MDGs 4,5,6 FAITH implemented the Comprehensive HIV and AIDS program and facilitate the delivery of services to the Injecting Drug Users in Kanchanpur district of Nepal with support from Save the Children, Nepal. The goal of the project is to reduce HIV transmission and enhance the quality of life of people living with HIV and AIDS and to contribute to the achievement of Millennium Development Goals 4, 5, 6. Major activities and outcomes: SN Particulars Target Achievement 1 BCC-IDU 170 157 2 # and % of new IDUs reached for the first time with Harm Reduction Program 162 157 3 Enabling Environment including Stigma and Discrimination, Reduction i Orientation to Police Personnel 45 65 ii Interaction meeting with Media Personnel 45 45 iii P/E training/ Refresher 1 1 iv Monthly PE Meeting 12 12 v Monthly Staff Meeting 12 12 24 24 4 (one each) 4 4 Refer to ARV, PMTCT, TB, CHBC, Hepatitis Diagnosed and Treatment Services (Only needy People) 5 Days Observation (AIDS, Condom, Candle Light and Drug Day) 6 Coordination/ linkages Meeting with DACC and Stakeholders 20 21 7 Target Group Discussion 60 60 8 Orientation to Community Member/ Clubs 45 45 9 Orientation to Family Members 60 60 10 School Orientation (# of participants) 225 285 7 11 DIC management committee meeting (#of meeting conducted) 3 3 12 Referral for Detox and Drug Treatment with emphasis to women drug users(# of IDUS referred) 6 6 13 Distribution of IEC materials 3,600 3,513 14 No. of Condom Distribution 30600 26865 15 Orientation Sessions in Major Factories for condoms promotion and Information of STI in Major Industrialized 60 16 Referral for VCT 48 55 17 IDUs (Message broadcasted through local FM) 300 300 18 Reduce Stigma Associated with HIV and Changing Discriminatory Attitudes and Behaviours 300 300 19 Promote Acceptance of PLHIVs in Community 300 300 20 Sensitization to Media Personnel on HIA and AIDS at Regional Level (# of participants) 20 22 Issues/challenges: Due to citizens negative attitudes towards IDUs programme we have been facing instability of DIC and EC offices. So we have been shifting DIC and EC here and there, time and again. Due to high mobility of TG and police harassment make us difficult to carry out program activities smoothly. Most of our target group belong from street base and they are highly interested to visit rehabilitation centre. Although there is very limited amount of budget for rehabilitation purpose. 3.3. Intensified early and increased TB case detection amongst children (0-14 years) Children are the least prioritized groups for TB case findings in Nepal. The increase case detection rate among the age group 15 – 49 indicates that TB among children is also increasing as any child living in a setting where there are people with infectious TB can become ill with TB, even if they are vaccinated. Children whose parents are HIV positive or who are HIV positive are more vulnerable to TB. The primary objective of the project was to detect additional TB cases among children between the age group (0-14) in low case finding districts. The primary target population of the proposed project were children (0-14) who were in immediate contact of TB positive, 8 Children Affected by AIDS (CABA) and whose parents were living with HIV. The ten project districts were Kavre, Kathmandu, Chitwan, Makwanpur, Parsa, Bara, Rautahat, Sarlahi Mahottari and Dhanusa. The timeline of implementation was 15 months – February 2013 to 15th July 2014. It was implemented in partnership with Sano Paila, local NGO based in Parsa. Major activities: Project sharing with the Tuberculosis Control Network (TBCN) partners to share project objective and gain their support for the project implementation. Conduct one-day coordination workshop with DHO, district level microscopic and treatment centres to share project objectives; establish coordination and linkages with each centre to ensure successful implementation. Identification of all sputum smear positive cases in each project district from DOTS centre and developed detailed of each case. Children of these patients and those in his/her surrounding will be traced out and screened for TB. Identification of HIV positives family to screen their children conducted in coordination with District AIDS Coordination Committee (DACC) and Voluntary Counselling and Testing (VCT) centres. Conducted an orientation to volunteers for contact tracing, screening, sputum collection, linkages of the suspected cases to the microscopic centre and the TB detected cases to the treatment centre (DOTS). Conducted training to develop capacity of health care providers in microscopic centres and treatment centres on child TB diagnosis and management issues in accordance with the NTP guidelines. Developed and distributed IEC materials on childhood TB to increase awareness, quality sputum and advocate for collaborative approach to increase childhood TB. Door to door volunteers mobilization with set targets based on the baseline of the respective districts to conduct screening and referral of all suspect cases. Conducted TB orientation program and screening in local schools with consent from teachers and parents. Conducted mobile microscopy camps in hard to reach areas that lie outside of the 10 km radius from an existing TB diagnosis facility. Conduct orientation workshops with heath workers who are directly providing safe motherhood services to sensitize them about childhood TB for the early detection of TB. Conduct a workshop with private practitioners (PPM) to enrol identified childhood TB case to the nearest NTP treatment centre. Dissemination workshop of lessons learnt with participation district, regional and national level among relevant stakeholders including Ministry of Health and Population, NTP, WHO and other TBCN partners. Major Outcomes: The project was officially launched in all 10 districts and the participants were well informed about the projects and they showed commitment to support the project. A total 363 volunteers were trained to conduct contact tracing, suspected case identification, sputum collection method, linkages of the suspected cases to the 9 microscopic centre and the TB detected cases to the treatment centre (DOTS). The completion of this orientation initiated the contact tracing and screening of cases in the field. Total 129 health care providers in microscopic centres and treatment centres were trained on child TB diagnosis and management issues in accordance with the NTP guidelines under this project. 10000 posters and brochure were developed in Nepali language and distributed through community volunteers, District health offices (DHO), health post, sub- health post and at the World TB day 2013 national event. It was used by the community volunteers mainly to create general awareness and as well as to give them the right information on TB to reduce stigma related with TB prevalent in the community. The project reached 7285 index cases and screened 19881 children through contract tracing. Total 29 SS+ and 184 all forms were identified and enrolled in the DOTS centre. A total 1000 CABA were screened out of which 16 TB cases were diagnosed and enrolled at their nearest DOTS centre. A total of 1083 school children were screened out of which 2 were diagnosed and treatment enrolled as TB cases. A total of 4133 children were screened through mobile camps out of which 14 SS+ and 91 all forms were diagnosed. The identified TB positive cases were referred for treatment and follow-up in the nearest health institution. Total 255 health personnel working in safe motherhood service are oriented to conduct TB screening. Total 1000 pregnant women and children under 5 years are screened for TB. Total of 96 general physicians and paediatricians are oriented on childhood TB program and diagnosis through this project. Total of 1416 children were screened out of which out of which 16 SS+ and 101 all forms cases were identified through this strategy and enrol in the DOTS centre from total project districts. Issues/challenges The NTP age wise TB recording and reporting system address only 0 – 8 years for all form of TB and children of the age group 8 – 15 years is address under the adult category. It has its direct adverse impact on the overall additionality of the project. High dependency in paediatrician or general physician for the diagnoses of TB among children, hence nearly 50 children who has M.T positive, X-ray suspected is still kept under observation. Lack of sensitive diagnostic tools like tools (Xpert®MTB/RIF, CX-R, ultra sound) to diagnose TB in most of the project districts. Migration and incomplete information about the index cases at the treatment centres. Also due to social stigma, index cases are difficult to approach. Most children are unavailable at home for screening because of their school so volunteers conduct screening at morning and evening time. It is compulsory to screen the children in presence of their guardian, as most of them are unable to describe their problem. Hence, to meet both of them together is also another challenge. It takes more time to take the suspected children to hospital for diagnosis. Their family members should accompany the suspected children to diagnostic centre which is not always feasible for all parents. 10 Success case study provided by Sano Paila – A little step TB DIAGNOSED IN THREE GENERATIONS (A Case Study) In Harpatgunj 2 of Parsa district, our volunteer encountered a farmer who is suffering from TB and is taking medicines from DOTS Center at Sirisiya Health Post. He is 26 years old living with his wife and three kids. His father had TB and died during the treatment. While tracing out his contacts, our volunteers found that his six year old son had cough and fever for more than 3 weeks. His condition gets worse during evening with mild fever. His parents told our volunteers that when their son coughed, they felt as if he was going to cough his lungs out and it really scared them. This symptom began to develop a month ago, informed the child’s father. “Our son had mild cough and fever in the beginning and I got medicines from the village medicine shop. When our son took the medicine, he felt good and the symptom disappeared, but when the dose was over, the symptom came back again,” added his father. As per the TB screening form, our volunteers collected three morning sputum samples of the child and referred him to microscopic center at Narayani Sub Regional Hospital in Birgunj. The sputum smear examination results revealed 4 AFB count in first 2 samples and confirmed that the child had TB. “This is a one in million case, a 6 year old child having sputum smear positive” was statement quoted by Dr. Shailesh Thakur, Pediatrician of Narayani Sub-Regional Hospital.” Now, the child is under TB medication at Sirisiya Health Post, Parsa District. He and his family were provided with basic health education on TB along with suggestions for nutritious diet intake. 4. ANNUAL MAJOR ACCOMPLISHMENTS: 1. Greater and meaningful participation of civil society organizations in national HIV and TB control program. 2. Involvement of community to contribute to decrease the burden of HIV and TB by creating awareness, advocacy and case findings. 3. Strengthen of collaboration with government bodies to address the burden of HIV and TB. 11 5. SUMMARY OF FINANCIAL DETAILS: S. No Project title Budget Expenditure Remarks Funding Agency Nepal Tuberculosis Centre (NTC)/GFATM, Bhaktapur Save the Children, Nepal /GFATM. WHO - TB REACH, Geneva 1. National Tuberculosis Programme (NTP) 8178000.00 7416575.00 Auditor’s payment balanced. 2. Nepal Round 10 Proposal to Contribute to the Achievement of MDGs 4,5,6 Intensified early and increased TB case detection amongst children (0-14 years) Grand Total in NRs 3304100.00 3020864.00 17610233.86 17610233.86 There was no deviation. There was no deviation. 29092333.86 28047673.59 3.