Section 504 Evaluation Report (D393043:1)
advertisement
")
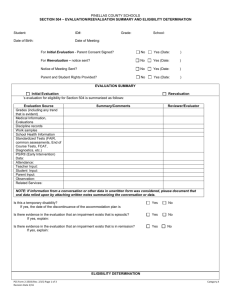
School District Evaluation/Reevaluation Report Section 504 of the Rehabilitation Act of 1973 Chapter 15 of the Regulations of the Pennsylvania State Board of Education _______________________________________ ____________________________________ Student name Age _______________________________________ ____________________________________ Parent/Guardian Name(s) Date written consent received Grade level Date of report ________________________________________________________________________________ Parent/Guardian address ________________________________________________________________________________ Second Parent/Guardian address (if form mailed separately) Disability Determination. If the answers to questions a. and c. are “yes,” or if the answers to question a., e., and g. are “yes,” the team must complete all sections of this report, to the extent applicable, and a service agreement must be developed for the child. If the answers questions, a. and e. are “yes,” but the answer to question g. is “no,” the team must complete only section 4 of this report, and a service agreement will not be developed. In such cases, however, the counselor to whom the child is assigned and the administrator responsible for enforcement of exclusionary discipline in the building to which the child is assigned, shall maintain, or have ready access to, a copy of this report. If the answer to question a. or question e. is “no,” the team must complete only section 4 of this report, and the parents of the child must receive notice that the child is not eligible for adaptations, modifications, services, or protections under Section 504 and Chapter 15. Section 1. a. Does this child have or continue to have a physical or mental impairment? □ yes □ no b. If “yes,” describe the impairment or impairments: c. Does the physical or mental impairment substantially limit a major life activity or activities related to school access or participation, whether academic, non-academic, or extracurricular, or does it continue to do so? □ yes □ no d. If “yes,” describe each major life activity that is or continues to be so limited and the effect that this limitation has on school access or participation, whether academic, non-academic, or extracurricular: e. If the physical or mental impairment does not substantially limit or no longer substantially limits a major life activity related to school access or participation, does the child take or use mitigating measures that ameliorate the effects of his or her impairment in school or school-related settings? □ yes □ no Form developed March 2010 f. If “yes,” describe those mitigating measures: g. If the child takes or uses mitigating measures that ameliorate the effects of his or her impairment in school or school-related settings, does he or she require assistance with the administration, monitoring, or application of these measures in academic, non-academic, or extracurricular settings? □ yes □ no Section 2. a. Present Levels of Academic and Functional Performance. Is this child meeting grade-level academic benchmarks? □ yes □ no b. If “no,” describe his present levels for each area in which he or she is not meeting gradelevel benchmarks and explain the cause(s) of below grade-level performance in each such area, and explain why this child does not require special education services under the Individuals with Disabilities Education Act (“IDEA”): c. Is the child demonstrating age-appropriate functioning and development in language and communication, social skills, behavior, and fine and gross motor skills? □ yes □ no d. If “no,” describe his present levels for each area in which he or she is not meeting ageappropriate benchmarks and explain the cause(s) of below grade-level functioning in each such area, and explain why this child does not require special education services under the IDEA: Section 3. Medical and Physiological Concerns. a. Does the child’s disability require that he or she receive ongoing or emergency medical care or treatment, including but not limited to the administration or monitoring the effects of medication, during school hours or during school-related activities? □ yes □ no b. If “yes,” describe the ongoing or emergency treatment required: c. If the child does require ongoing or emergency medical treatment, does the District have in its possession current, clear orders from a licensed physician for each aspect of the required treatment? □ yes □ no Form developed March 2010 2 d. If “no,” describe those aspects of required ongoing or emergency treatment for which current, clear orders are needed and a plan for obtaining them from the treating physician of the child or from a physician appointed for that purpose by the District: Section 4. Test and Assessment Results. a. Summarize all testing and assessments that the team conducted or reviewed to support (1) its determination of whether the child has or continues to have a disability and (2) if applicable, its assessment of the child’s present academic and functional levels and needs. Include any norm-referenced, criterion-referenced, and curriculum-based assessments; functional behavioral assessments; observations; work samples reviews; and progress monitoring or benchmark assessments in the summary, and reconcile or explain, if possible, any inconsistencies in these sources of information: b. Explain the extent to which the team relied on standardized testing that was not conducted under the standardized conditions prescribed by the publisher of the test, and how the results thus obtained were interpreted and used. Section 5. Recommendations. Identify any adaptations, modifications, services, or ongoing or emergency medical treatment that the team recommends as necessary, as a result of the identified disability or disabilities of the child, to access and participate in academic, non-academic, and extracurricular programs and services: Section 6. Signatures of Team Participants. The signature, printed name, and position of each team member below indicate that the identified team member participated in or contributed to this evaluation or reevaluation. Signatures do not indicate agreement or disagreement with any aspect of this report. ______________________________________________________________________________ Signature Printed Name Title or Position ______________________________________________________________________________ Signature Printed Name Title or Position ______________________________________________________________________________ Signature Printed Name Title or Position ______________________________________________________________________________ Signature Printed Name Title or Position ______________________________________________________________________________ Signature Form developed March 2010 Printed Name Title or Position 3