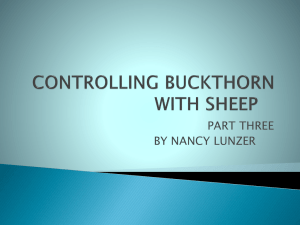
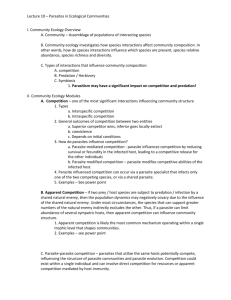
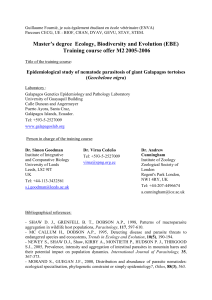
Blood Parasite Smear
advertisement

SMILE Blood Parasite Smear- Giemsa Stain Blood Parasite Smear- Giemsa Stain Document Number: Effective (or Post) Date: Date of last review: Reviewed by: Author: Penny Stevens Review History Pro67-D-01 17 February 2009 11 May 2010 Heidi Hanes SMILE Comments: This document is provided as an example only. It must be revised to accurately reflect your lab’s specific processes and/or specific protocol requirements. Users are directed to countercheck facts when considering their use in other applications. If you have any questions contact SMILE. Penny Stevens Procedure Number Date International QC/QA Coordinator Pro6.7-D-01 Version 1 May-05 Author(s), Name & Title Name, Title Signature Date Name, Title Signature Date Approved By SOP Annual Review Version # [0.0] Revision History Name (or location) Distributed Copies to Associated Forms: 106731517 Revision Date [dd/mm/yy] Description (notes) # of copies Name (or location) # of copies SMILE Blood Parasite Smear-Giemsa Stain I acknowledge that I have read, understand and agree to follow this SOP. Name (print) 106731517 Signature Date SMILE Blood Parasite Smear-Giemsa Stain Copy _____ of ___ Effective Date: HEMATOLOGY SECTION C. DIFFERENTIAL CELL COUNTS C.5. BLOOD PARASITE SMEAR/GIEMSA STAIN C.5.1. PRINCIPLE: The diagnosis of blood parasites is based on the demonstration of the organism in the blood. The preparation of thick and thin blood films, the appropriate use of stains, and the detection and identification of parasites are crucial to clinical diagnosis of many parasitic diseases. The following is a list of the blood-borne parasitic diseases that may be encountered in the hematology laboratory: 1. Malaria 1.1. Plasmodium are transmitted to man by the bite of the Anopheles mosquito. Fever is the clinical manifestation of malaria, and the patient's admission diagnosis is often “fever of unknown origin”. The rational treatment of malaria requires, however, that both the existence of malaria and the type of malaria be established in the laboratory. Dates and place(s) of travel to endemic areas are required to establish the diagnosis, if malaria infection is suspected. 2. Babesiosis (Babesia species) 3. Trypanosoma 1. Chagas’ Disease (Trypanosoma cruzi) 2. African Trypanosomiasis (T. brucei, T. gambiense, T. rhodesiense) 4. Filariasis (W. bancrofti, B. malayi, L. loa) C.5.2. SPECIMEN COLLECTION: 1. The optimum time for specimen collection for parasitologic examination varies with the particular parasite suspected. Therefore, the following factors must be taken into consideration when selecting the optimum time to prepare smears: 106731517 SMILE Blood Parasite Smear-Giemsa Stain 1.1. Malaria 1.1.1. The best time to obtain blood for smears is about midway between chills to ensure obtaining stages on which species identifications can be made. PERFORM BLOOD COLLECTION IMMEDIATELY UPON FIRST SUSPICION OF MALARIA. 1.1.2. Single films may not reveal organisms, therefore NCCLS recommends successive smears prepared and examined every six (6) to eight (8) hours for up to three days. 1.1.3. Blood samples must be taken BEFORE any anti-malarial drugs are used to ensure demonstration of organisms if the patient does have malaria. 1.2. Babesiosis 1.2.1. Diagnostic methods are similar to malaria and organisms may be found at any time of the day. 1.2.2. Single films may not reveal organisms, therefore successive films every six (6) to eight (8) hours for up to three (3) days are recommended. 1.3. Chagas’ Disease Trypomastigotes are generally seen in circulating blood during the early acute phase (the first month of infection) and in subsequent febrile periods. Films prepared at other times are of little diagnostic value. 1.4. African Trypanosomiasis Organisms are present in the blood during the acute phase of infection. After several months to a year, they are better demonstrated in spinal fluid. 1.5. Filariasis 1.5.1. Microfilariae, Wuchereria bancrofti and Brugia malayi, show nocturnal periodicity. Prepare films at night, usually around midnight. 1.5.2. Microfilariae, Loa loa, show diurnal periodicity. Prepare films at noon. 1.5.3. The suggested nocturnal and diurnal collection times suggest that the patient has been in the present time zone for a period of time sufficient for the parasites to have adjusted to the patient’s present 24-hour activity cycle. Therefore, it may be necessary to draw blood at ‘off’ hours to coincide with the appropriate periodicity for patients who have recently returned from endemic areas. The other species are considered non-periodic and films may be made at any hour. 106731517 SMILE Blood Parasite Smear-Giemsa Stain 1.5.4. Microfilaremias (unless in nationals in endemic areas) are lower in most Americans and Europeans, who become infected, and simple thin and thick films may not allow detection of organism. Other methods of detection, not currently performed in this laboratory, may be required. 2. Blood Collection by Skin Puncture 2.1. Finger punctures using the palmar surface of the tip of the finger are preferred for parasite blood films. The middle or “ring” fingers are generally used but the heel may be used as well. 2.1.1 Palmar surface of the distal phalanx of a finger. 2.1.1.1. The puncture must be on the palmar surface of the distal phalanx and not at the side or tip of the finger. 2.1.1.2. The middle and ring (fourth) fingers are the preferred sites. 2.1.2. Lateral or medial plantar surface of the heel (infant specimens only) 2.1.2.1. If an infant’s heel is to be punctured, the site must be on the plantar surface medial to a line drawn posteriorly from the middle of the great toe to the heel or lateral to a line drawn posteriorly between the 4th and 5th toes to the heel. The puncture must not be through a previous site, which may be infected, nor should it be at the curvature of the heel. 2.1.2.2. Excessive crying may adversely affect the concentration of some constituents (e.g., leukocyte count). If possible, a waiting period of 30 minutes should be observed between the time crying ceases and the performance of the skin puncture. If specimen is collected while patient is crying, note the condition on the report. 2.1.2.3. Skin puncture must not be performed on the central area of an infants foot nor on the fingers. 2.1.2.4. The puncture site should be warm to the touch. Do not perform the procedure on swollen puncture sites, because accumulated fluid will contaminate the blood specimen. 2.1.3. The technique for puncturing the finger or heel is to prick the skin with a sterile, nonreusable lancet deeply enough to allow collection of a sufficient amount of freeflowing blood to prepare thick and thin films. After collection, pressure should be applied to the puncture site with cotton or gauze until bleeding stops. Bandage the site and do use an alcohol wipe after puncture, as this will prolong the bleeding. 106731517 SMILE Blood Parasite Smear-Giemsa Stain 2.1.4. Refer to the Specimen Collection and Processing Section Skin Puncture SOP for diagrams or more information. 2.2. Thick film preparation from finger puncture. Prepare four (4) films as follows: 2.2.1. The contact method is the preferred method. The ideal thick film will be the size of a dime (1.5 to 2.0 cm diameter) and just thick enough so that newsprint can barely be read through it. The most common error is using too large of a drop of blood. 2.2.1.1. Touch the slide to the drop of blood, which should be rounded up on the finger or heel. 2.2.1.2. Spread with an applicator stick. 2.2.2. The puddle method may also be used but may result in parasite distortion. 2.2.2.1. Collect two to three small drops of blood by touching the slide to the blood on the finger. Do not milk the finger. 2.2.2.2. Use an applicator stick to combine the separate pools into one puddle to form a thick film of appropriate size and density. 2.2.2.3. Stir the puddle for 30 seconds to remove fibrin strands. 2.2.3. Prepare four (4) slides using either method. Label slides with a pencil and dry horizontally at room temperature. 2.3. Thin film preparation from finger puncture. Prepare four (4) films as follows: 2.3.1. Collect a small drop of blood by touching the slide to the blood on the finger. 2.3.2. Immediately perform a routine wedge blood smear procedure to prepare four (4) thin smears. The drop of blood for the thin smear should be large enough to provide a thin film with a "tongue" or thin tapering towards the center of the slide and a feathered edge. Specimens containing streamers of blood (caused by chipped spreader slides), streaks (caused by dirt) and holes (caused by grease) are unacceptable. 2.3.3. Prepare four (4) slides using either method. Label slides with a pencil and dry horizontally at room temperature. 3. Venipuncture 3.1. 106731517 Venipuncture is not recommended for blood film preparation for parasite examination. However, collect one EDTA specimen by venipuncture for internal CBC test evaluation. If the physician did not order the CBC, perform the test but do not order or report the results in [your SMILE Blood Parasite Smear-Giemsa Stain laboratory system]. If the venipuncture method is also used for slide preparation, annotate why on the blood parasite result form. 3.2.1. Do not use under filled specimens. Under filled tubes may interfere with blood to slide adhesion during smear preparation and improper parasite staining. 3.2.2. Prepare slides within two (2) hours of specimen collection. 3.2. Slide preparation 3.2.1. Thick film 3.2.1.1. Place one large drop of well-mixed blood in the center of a glass slide. 3.2.1.2. Carefully spread the drop of blood. The preferred thick film will be the size of a dime (1.5 to 2.0 cm diameter) and just thick enough so that newsprint can barely be read through it. The most common error is using too large of a drop of blood. Prepare four (4) thick smears. 3.2.2. Thin film Perform a routine wedge blood smear procedure to prepare four (4) thin smears. The drop of blood for the thin smear should be large enough to provide a thin film with a "tongue" or thin tapering towards the center of the slide and a feathered edge. Specimens containing streamers of blood (caused by chipped spreader slides), streaks (caused by dirt) and holes (caused by grease) are unacceptable. 3.2.3. Prepare four (4) slides. Label slides with a pencil and dry horizontally at room temperature. C.5.3. EQUIPMENT & REAGENTS: 1. EQUIPMENT: 1.1. Glass slides 1.2. Filter paper (Do not use gauze) 1.3. Cool air dryer 1.4. Microscope 1.5. 100X Oil immersion lens 106731517 SMILE Blood Parasite Smear-Giemsa Stain 1.6. Wooden applicators 1.7. Clean gauze or tissue 1.8. Three (3) coplin jars 1.9. 50 mL class A graduated cylinder 1.10. Timer 1.11. Forceps 1.11. [your laboratory system] labels 1.13. Blood Parasites result form 2. REAGENTS: 2.1. Filtered Wright-Giemsa stain 2.2. Absolute Methyl Alcohol 2.3. Buffer (pH 6.8-7.2) 2.4. Triton X-100 5% solution C.5.4. CALIBRATION: Not applicable. C.5.5. QUALITY CONTROL: 1. To ensure that proper staining results have been achieved, prepare a positive smear (malaria) with each new batch of working Wright-Giemsa stain. Select an EDTA specimen that displays at least one parasite in every 2 to 3 fields. If available, use prepared frozen positive control slides. 2. If control slides are unavailable, use a normal blood smear (submitted for white blood cell differential count) to check the quality of staining prior to staining patient smears. 3. Control slides will be prepared from positive patient’s blood and stored for future use as follows: Prepare as many thin smears as possible within one hour of specimen collection. Allow the smears to dry quickly, using a fan or blower at room temperature. Fix the smears in absolute (100%) methanol for one minute and allow them to dry. Place them back-to-back in a box with separating grooves. 106731517 SMILE Blood Parasite Smear-Giemsa Stain Label the outside of the box with date, species and “Giemsa + control”. Store at -70°C or colder indefinitely. Blood films stored at warmer temperatures will not maintain good staining characteristics. When needed, remove the smear from the box, allow the condensation to evaporate and label the slide with “+ malaria” and the present date. The smear is now ready for staining since it was previously fixed. 4. ACCEPTABLE QC LIMITS: 4.1 Macroscopic Evaluation – Stained blood smears appear purplish. If the smear appears blue, the buffered water was too alkaline, and if the smear appears pink, the buffered water was too acidic. 4.2 Microscopic Evaluation 4.2.1 RBC’s should appear buff-pink to pale bluish-gray, with no artifacts due to stain precipitate or water from incomplete fixation. 4.2.2. Platelets have a pale blue cytoplasm and diffuse red nuclear material. 4.2.3. Neutrophils should have a purple nucleus and pink granules. 4.2.4. Lymphocytes and Monocytes should have a purple nucleus and a pale blue-gray cytoplasm. 4.2.5. Eosinophils should have coarse pink granules in the cytoplasm. 4.2.6. Basophils should have coarse, deep blue granules in the cytoplasm. 5. DOCUMENTATION. Annotate quality control (QC) as satisfactory or unsatisfactory on the Giemsa Stain QC form based on the above criteria. (Appendix 3) C.5.6. PROCEDURE: 1. REAGENT AND PREPARATION 1.1. PHOSPHATE BUFFERED SALINE (PBS) PREPARATION: 1.1.1. Store the PBS powder at room temperature in the flame cabinet. 1.1.2. Dissolve the contents of one (1) vial in 3.8L (1 gal) of deoinized or distilled water to prepare buffer, 8.3 mmol/L, pH 6.8 – 7.2. Label accordingly with reconstitution date and tech initials. Annotate the expiration date as the same as the water stock ‘or When turbid’. 106731517 SMILE Blood Parasite Smear-Giemsa Stain 1.1.3. Test the pH with pH indicator strips. Ensure that the pH reads 6.8 – 7.2 before use or storage. 1.1.4. Once reconstituted, store the PBS in the refrigerator at 2-6oC. Discard if turbidity develops. 1.2 TRITON X-100 5% SOLUTION Prepare five (5) percent solution and store reagent in a 30 mL dropper bottle in the flame cabinet. 1.2.1. Use the following formula to calculate the volume of stock solution necessary (V1): (C2 x V2)/C1 = V1 Where C1 = % stock solution concentration, V2 = total volume desired and C2 = 5% (the desired concentration). 1.2.2. Example: To make 30 mL of a 5% solution from a 20% stock solution: (5 x 30)/20 = V1 V1 = 7.5 mL 1.2.3. Dilute up to the desired concentration with reagent grade water. In example 2.1.2 you would use 30 mL – 7.5 mL = 22.5 mL’s of reagent grade water. 1.2.4. Due to supplier availability, the stock solution may be ten (10) or twenty (20) percent. Do not use concentrated Triton X-100 as it is difficult to get into solution. 1.3. FILTERED WRIGHT-GIEMSA Filter the stock stain with one Whatman© Filter into labeled glass reagent jar. Use only filtered stain for blood parasite testing. 2. STAIN PROCEDURE (15 Minute 7.5% Stain) 2.1. Prepare specimens as directed previously. 2.2. 2.3. Collect the required equipment as identified in section 5.3.1. Obtain one (1) QC slide as indicated in section C.5.5. They are stored in a slide box in the Hematology/Chemistry freezer. 2.4. Rinse the coplin jars with the solution that they will contain before using. Rinse the graduated cylinder with PBS. 2.5. Prepare a 7.5 percent (working) Modified Wright Giemsa. Working stain must be prepared fresh daily. 106731517 SMILE Blood Parasite Smear-Giemsa Stain 2.5.1. Add the following to the fifty (50) mL graduated cylinder: 2.5.1.1. 37 mL’s PBS. Check the pH using pH indicator strips and annotate the pH on the QC chart. (see appendix 3) The pH must be 6.8 to 7.2. If the pH is out or the solution is cloudy, open a fresh bottle or prepare fresh PBS solution. 2.5.1.2. 3 mL’s of pre-filtered Giemsa stain. 2.5.1.3. 2 drops of 5% Triton X-100 2.5.2. Pour the mixture into the designated coplin jar and mix well with a disposable pipette. 2.6. Prepare a Triton X-100 buffer rinse solution. 2.6.1. Pour 45 mL’s of PBS buffer into a clean (PBS rinsed) coplin jar. 2.6.2. Add two (2) drops of Triton X-100. 2.6.3. Mix well with a disposable pipette. 2.7. Fix two (2) thin smears in a methanol filled coplin jar for one (1) minute and allow them to air dry vertically. DO NOT FIX THE THICK SMEARS!! 2.8. Place the QC slide, the fixed thin smears and two (2) thick films into the (working) Modified Wright Giemsa. Stain for 15 minutes. 2.9. At the end of staining time, remove each slide individually, starting with the thick film, and drain briefly onto gauze. Do not allow the slides to dry. 2.10. Place the thick films into the prepared Triton X-100 buffer solution and set a timer for five (5) minutes (see step 2.6). 2.11. Rinse the thin smears briefly by dipping in and out of the same buffer solution until the slide runs clear (3-5 dips). 2.12. Remove the thick films after five minutes, taking care not to wash the specimen off the slide, and allow them to dry vertically. 2.13. Read the slides as indicated in section C.5.7. Read the QC slide first and annotate stain quality on the Giemsa stain form. (see appendix 3) 2.14. Complete the Blood Parasites worksheet. (see appendix 4) 106731517 SMILE Blood Parasite Smear-Giemsa Stain 2.15. Result in [your laboratory system] as indicated in section C.5.7. Reporting. 2.16. Place all eight (8) slides, Blood Parasites Worksheet and CBC Cell-Dyn report (see section C.5.2. Venipuncture 3.3.1. for more information) into a slide folder. Add the appropriate additional testing and notify the day shift personnel. 2.17. Clean the glassware Do not allow the glassware to soak in tap water. Tap water is not sterile and results in mineral deposits, which can affect the buffered pH of the water and stain. 2.17.1. Wash all glassware immediately with tap water and hand soap. 2.17.2. Clean the Giemsa coplin jar with methanol. Dispose of waste methanol appropriately in microbiology. 2.17.3. Rinse well with tap water. 2.17.4. Perform a final rinse with REAGENT GRADE water and air dry. C.5.7. INTERPRETATION 1. THICK FILM EVALUATION 1.1. Scan the thick film briefly using the 10x objective searching for large forms such as microfilariae, schizonts and gametocytes. 1.2. Perform a thorough examination of at least 300 fields searching for parasite using the 100x oil immersion objective. 1.3. Staining Properties: 1.3.1. Macroscopic – A stained smear appears faint bluish-purple and is semi-transparent. (If the smear was fixed the stained smear will be dark purple and non-transparent. Note: Do not fix thick smears.) 1.3.2. Microscopic 1.3.2.1. Erythrocytes will be dissolved and few ghost-like remnants may be present. (If the smear was fixed, the RBC’s will be intact and adhered to the slide. Note: Do not fix thick smears.) 1.3.2.2. Leukocytes have dark purple-blue nuclei and lighter cytoplasm, which is often indistinguishable. Eosinophil granules are bright pinkish-red and neutrophil/basophil granules are purple. 106731517 SMILE Blood Parasite Smear-Giemsa Stain 1.3.2.3. Platelets appear dark pink 2. THIN FILM EVALUATION: 2.1. Scan the thin film briefly using the 10x objective searching for large forms such as microfilariae, schizonts and gametocytes. 2.2. If the thick film was negative, examine the thin film thoroughly for five (5) minutes searching for parasites using the 100x oil immersion objective. 2.3. If the thick film was positive, use the thin film to isolate and identify genus only and to perform the parasitemia calculation, if required. See paragraph 4. 2.4. Staining properties: 2.4.1. Erythrocytes stain buff pink to pale bluish-gray. 2.4.2. Leukocytes: 2.4.2.1. PMN’s, monocytes and lymphocytes have a pale blue-gray cytoplasm and purple nucleus. 2.4.2.2. Eosinophils have coarse, pink granules in the cytoplasm. 2.4.2.3. Basophils have coarse, deep blue granules in the cytoplasm. 2.4.3. Platelets have pale blue cytoplasm and diffuse red nuclear material. Note that these are often mistaken for malaria parasites, especially if they are seen overlying an erythrocyte. 3. PARASITE IDENTIFICATION 3.1. Characteristics of Plasmodium Species: 3.1.1. In the thick smear, the erythrocytes are lysed and the parasite is seen free in a background of cellular debris. Look for the purple/blue ring form surrounding a red chromatin dot and any other stages as identified in appendix 7. 3.1.2. The thin smear has organisms within the red blood cell and is much less commonly seen than in the thick smear. 3.1.3. For identification specifics, refer to the following appendix documents: 3.1.3.1. Laboratory approach to Identification of Plasmodium species, Speciation Guideline. (See appendix 5) 3.1.3.2. Refer to table 1 for identification characteristics of Plasmodium species. (See appendix 6) 106731517 SMILE Blood Parasite Smear-Giemsa Stain 3.1.3.2. Refer to figure 1 for the morphology diagram. (See appendix 7) 3.1.4. The pathologist will perform speciation. 3.2. Characteristics of Babesia Species: 3.2.1. Diagnosis is usually made by detecting the intraerythrocytic parasite inclusions, which appear as tiny rings, ranging between 1.0 and 3.0 micrometers (m). They resemble the early trophozoites of P. falciparum. The nuclei are very small and one or two chromatin dots may be seen. Mature forms appear as doublets, simulating rabbit ears; or in tetrads, resembling a Maltese cross. The erythrocytes are not enlarged, are normochromic and do not develop stippling. 3.2.2. Refer to Table 3 for a comparison of Plasmodium falciparum and Babesia Parasites. (See appendix 8) 3.3. Characteristics of Hemoflagellates (Trypanosoma): 3.3.1. Trypanosoma gambiense and Trypanosoma rhodesiense The organisms are long, slender, spindle-shaped forms, measuring 15-30 micrometers (m) in length and 1.5-4 micrometers (m) in width. A single flagellum takes its origin from a dotlike kinetoplast located posterior to the central nucleus. The flagellum runs along an undulating membrane the projects beyond the anterior point of the organism. 3.3.2. Trypanosoma cruzi The circulating trypanosomal organisms are similar to those of T. gambiense and T. rhodesiense. Characteristic C-forms are characteristic when seen, but are rarely diagnostic. 3.4. Identification of Microfilariae 3.4.1. Wuchereria bancrofti Organism measures 245-449 micrometers (m) in length x 7.5-10 micrometers (m) width, these forms can easily be seen in direct microscopic examinations of blood, especially when collected at night. This microfilariae has a sheath and the column of nuclei terminate 15-20 micrometers (m) proximal to the tail, leaving a clear space. 3.4.2. Brugia malayi Organism appears similar to those of W. bancrofti and is also released into the bloodstream with nocturnal periodicity. They differ from W. bancrofti in that 2 nuclei, 106731517 SMILE Blood Parasite Smear-Giemsa Stain spaced about 10 micrometers (m) apart from the main column, extend into the tip of the tail. 3.4.3. Loa loa Organism appears similar to those of W. bancrofti and B. malayi, except that the column of nuclei extends completely to the tip of the tail section. A sheath is present. Adult worms release the microfilariae on a diurnal schedule. 4. Plasmodium PARASITEMIA DETERMINATION 4.1. Determination of parasitemia becomes important when therapy is initiated. The patient’s parasitemia is monitored so that possible cases involving drug-resistant strains of P. falciparum may be detected. Parasitemia should be performed at 24, 48 and 72 hours after initiating therapy. Generally, if the malarial strain is susceptible to the therapeutic regimen, the parasitemia will drop significantly within the first 24 hours (often by 50% or more). 4.2. Parasitemia will be performed on all positive Plasmodium and Babesia cases and the parasitemia percentage reported as indicated below. Use the manual cell counter for this procedure. 4.2.1. Procedure: 4.2.1.1. Count the RBC’s in a minimum of 10 fields using 100x on the thin smear using a manual cell counter. 4.2.2.2. Using a different counter, at the same time, count the number of malarial parasites. Count only those parasites that are intraerythrocyte (inside the RBC’s). An infected RBC will be counted once using the RBC counter and once using the malaria counter. 4.2.2.3. Report the percent (%) parasitemia as the percentage of infected RBC’s per 100 RBC’s counted. Carry the decimal out two places and always round appropriately. 4.2.2. Calculation Example: 4.2.2.1. 25 parasites counted per 1000 RBC’s 4.2.2.2. (25/1000) x 100 = 2.50% Parasitemia C.5.8 REPORT PROCEDURES 1. REPORT PROCEDURE: 106731517 SMILE Blood Parasite Smear-Giemsa Stain If a blood parasite (Malaria) test is requested on evening or weekend shifts, trained shift personnel MUST PERFORM TESTING AND CERTIFY RESULTS ON THEIR SHIFT. 1.1. Positive Results 1.1.1. Notify the appropriate physician immediately. 1.1.2. Notify the pathologist immediately. 1.1.3. Certify the result as indicated in the report format section 2.1. 1.1.4. Add a pathologist review to all POSITIVE malaria reports. 1.2. Negative Results 1.2.1. Certify the result as indicated in the report format section 2.2. 1.2.2. Add a supervisor review to all NEGATIVE malaria reports. 2. REPORT FORMAT: 2.1. Unquestionable Positive malaria smears will have many malarial parasites on the thick and thin smears and more than one intraerythrocyte parasite observed on the thin smear. Positive results will be entered as PM with the following free text and canned comments added: 2.1.1. [PDP] – “Preliminary diagnosis: POSITIVE for Plasmodium. 2.1.2. % Parasitemia (See paragraph 5.7.4. for procedure) 2.1.3. “Critical Result telephoned to” followed by the name of the physician notified and the date and time of notification. 2.1.4. [PP] –“Pending final review by pathologist.” 2.2. Negative parasite results Negative for ALL parasites will be entered NM with the following free text comments added: 2.2.1. Preliminary diagnosis: Negative for Blood Parasites. 2.2.2. “Pending final review by Supervisor.” 106731517 SMILE Blood Parasite Smear-Giemsa Stain 2.3. Unquestionable Positive smears, NOT Plasmodium will have many parasites on the thick and thin smears. Positive results will be entered as PO& with the following free text and canned comments added: 2.3.1. Preliminary diagnosis: Positive for blood parasites, Not Plasmodium. 2.3.2. Identify the Genus present: Trypanosoma or Microfilaria 2.3.3. “Critical Result telephoned to” followed by the name of the physician notified and the date and time of notification. 2.3.4. [PP] -Pending final review by pathologist.” 2.4. Questionable interpretation 2.4.1. Enter SEE BELOW& with the following free text comments: 2.4.1.2. Preliminary Diagnosis Indeterminate. 2.4.1.2. Pending review by supervisor or pathologist. 2.4.2. Notify the physician that the result is questionable and requires supervisor confirmation or determination. Annotate the notification using a free text comment and CERTIFY THE RESULT. The supervisor or pathologist will certify their own results under their SUP or PATH test. 2.4.3. Call the supervisor or pathologist immediately to perform testing. 3. Blood parasite infection cannot be ruled out by a single negative blood sample. Multiple Blood films from different blood draws are required before any patient can be considered “negative” for blood parasites. 4. Pathologist reviews are not performed STAT, unless requested by the clinician, notify the pathologist immediately for all ‘STAT’ readings. 5. All positive blood parasite results are considered critical. Notify the clinician immediately and annotate according to the Critical Results SOP in [your laboratory system]. Notify the pathologist immediately for review of slides and speciation. 6. The pathologist will perform the final review on ALL POSITIVE results. C.5.9. CALCULATIONS: See sections C.5.6. 5% Triton X-100 and C.5.7. Parasitemia Determination 106731517 SMILE Blood Parasite Smear-Giemsa Stain C.5.10. PROCEDURAL NOTES: 1. The clinical manifestations caused by the Plasmodium parasites are fundamentally different: 1.1. P. falciparum infection diagnosis is a medical emergency and requires rapid identification because infection with this organism is always potentially fatal without immediate treatment. 1.2. P. malariae is also important because it can cause, in some but not all, an immune complex disease associated with nephrotic syndrome and the risk of renal failure. 1.3. P. vivax and P. ovale are responsible for a vast amount of febrile illnesses in endemic areas. 2. Universal precautions will be used when handling all specimens to include those suspected of bloodborne pathogens. C.5.11. APPENDICES: 1. SOP Validation Form and SOP Change Control 2. SOP Approval 3. Quality Control/Manual Wright Giemsa Stain Form 4. Blood Parasites Worksheet 5. Laboratory approach to Identification of Plasmodium species, Speciation Guideline 6. Identification Characteristics of Plasmodium Species. NCCLS 2004 M15-A Vol. 20:12, pg. 21 Table 1 7. Color chart diagram of Plasmodium species erythrocytic stages 8. Morphological Characteristics of Plasmodium falciparum and Babesia species, NCCLS 2004 M15-A Vol. 20:12, pg. 24 Table 3 C.5.12. REFERENCES: 1. Despommier, D., Gwadz, R., and Hotez, Peter J.: Parasitic Diseases, Third Edition, Springer-Verlag, New York, Inc. 1995 , Pages 174-189. 2. CDC-Division of Parasitic Diseases: DPDx, Identification and Diagnosis of Parasites of Public Health Concern; http://www.dpd.cdc.gov. 5 Nov 2001. 3. NCCLS. Laboratory Diagnosis of Blood-borne Parasitic Diseases; Approved Guideline. NCCLS 2004 document M15-A, Vol. 20 No. 12. 4. Brown, Barbara C.; Hematology; Principles and Procedures; Sixth Edition; Lea and Febriger Book Publisher; 1993; Pages 98-102 and 145-149. 106731517 SMILE Blood Parasite Smear-Giemsa Stain 5. Koneman, Elmer W.; Color Atlas and Textbook of Diagnostic Microbiology, Fifth Edition, LippencottRaven Publishers; 1997; pages 1121 – 1133 6. Sigma diagnostics Accustain Giemsa Stain, Modified. Package Insert. 106731517 SMILE Blood Parasite Smear-Giemsa Stain Appendix 1 SOP VALIDATION SOP NAME: Examination of Blood for Malaria Parasites Clear and specific title and principle: Comments: yes / no All necessary supplies, equipment, and materials are listed: Comments: yes / no SOP is sufficiently detailed to be understood but not overly complex: Comments: SOP text adequately describes process/procedure: Comments: SOP accomplishes purpose: Comments: yes / no yes / no yes / no Reviewed by: (Name & Title) Signature: ________________________ Date: __________________ SOP CHANGE CONTROL Date 106731517 Change QA OIC Med. Dir. SMILE Blood Parasite Smear-Giemsa Stain Appendix 2 SOP APPROVAL SIGNATURE DATE PREPARER QA COORDINATOR LABORATORY OIC MEDICAL DIRECTOR ANNUAL REVIEW REVIEWER SIGNATURE DOCUMENT COPY CONTROL LOCATIONS SUPERSEDES: ______________ DATE SOP RETIRED: ___________ 106731517 DATE REVIEWER SIGNATURE DATE DATE: ___________# COPIES __________ SMILE Blood Parasite Smear- Giemsa Stain Appendix 3 PREVENTIVE MAINTENANCE / QUALITY CONTROL WRIGHT-GIEMSA (WORKING) STAIN / BLOOD PARASITES QC Month: ____________ HEMATOLOGY SECTION MAINTENANCE Date 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 PBS pH (6.8 - 7.2) 15 Minute Stain Review for QC slide for Color, Precipitation & Contamination. Indicate SAT or UNSAT (see below) Positive QC Slide Prepared? Annotate YES or NO Organism identified on positive QC slide? Annotate YES, NO or N/A. Technician Initials PROTOCOL Giema Stain: Lot# ___________________________ Expiration Date:______________________ Buffer MFG:_____________ Lot# ___________________________ Expiration Date:______________________ YEAR: __________ 23 24 25 26 27 28 29 30 Note: See SOP C.5 Examination of Blood Parasites. Properly stained smears appear as follows: a) RBC's: Buff Pink to Pale Blue Grey b) WBC Nucleus: Dark purple c) WBC Cytoplasm: Neutrophil - light pink granules lymphoctes & monocytes - pale blue grey basophil - course, deep blue granules eosinophils - coarse pink granules d) Platelets have a pale blue cytoplasm and diffuse red nuclear material e) Zero to few stain precipitation particles present Comments/Problems and Corrective Action Supervisor Review:_________________________________________________________________ 106731517 Date:______________________ 31 SMILE Blood Parasite Smear- Giemsa Stain Appendix 4 BLOOD PARASITES WORKSHEET TIME RECEIVED: ________________ Place one large LIS label here TECH : __________________________ 1. Number of slides received: Thin __________________ 2. Slide preparation method: Contact / Puddle or other:______________________________ 3. Films properly prepared? YES or NO 4. EDTA specimen received? YES or NO 5. CBC performed & results attached: YES or NO 6. PARASITE RESULTS POSITIVE or Thick _______________ 6.1. Parasite Present: NEGATIVE 6.2. Parasite Type (key features): ___________________________________________________ _________________________________________________________________________________ _________________________________________________________________________________ 7. PARASITEMIA (Perform if Plasmodium/Babesia species or indicate if not applicable): N/A 7.1. Count a minimum of 10 fields on the thin smear. 7.2. Number of intraerythrocyte parasites: _________ 7.3. Calculation (number of parasites/number of RBCs) x 100: Number of RBCs:____________ (_____________/____________) x 100 = _______________ % Parasitemia 8. COMMENTS or [CR] NOTIFICATION_______________________________________________ __________________________________________________________________________________ 9. SUP REVIEW (Negative Results): ___________________________________________________ _________________________________________________________________________________ 10. PATH REVIEW (Positive Only): P. falciparum Non-P. falciparum Double Infection Other _________________________________________________________________________________ _________________________________________________________________________________ SUP or PATH SIGNATURE: 106731517 _____________________________ DATE: ___________________ SMILE Blood Parasite Smear-Giemsa Stain Appendix 5 LABORATORY APPROACH TO THE IDENTIFICATION OF PLASMODIUM SPECIES 1. IDENTIFY P. falciparum Tiny ring forms that occupy less than one third the diameter of the erythrocyte. Multiple forms present within one erythrocyte; with two nuclei in the same ring. Heavy infection, involving 20% or more of the erythrocytes. Appliqué effect - tiny rings plastered on the erythrocyte cell membrane. Infection typically occurs in erythrocytes of any age. Developing ring forms and schizonts are NOT present. These forms are usually ONLY present in terminal, fulminant P. falciparum infections. Banana or crescent shaped gametocytes are present. These are usually absent in early infection and begin to appear 7 – 10 days after the onset of fever. 2. MAKE AN OBJECTIVE ID OF P. vivax Infected erythrocytes are somewhat irregular in shape, enlarged, pale and contain prominent pink-red staining granules called schuffner’s dots. Infection typically occurs in young erythrocytes. All stages of ring forms may be present. Young rings measure larger than one third the diameter of the infected RBC. As the trophozites mature, they begin to fill the erythrocyte with “flowing” or “ameboid” cytoplasm. More than one nucleus is evident in preparation for the formation of segmented forms, known as schizonts. P. vivax schizonts comprise 12 – 14 or more individual segments, known as merozoites. Large circular gametocytes present. (A gametocyte is any single celled nucleus that occupies more than one-half the cell diameter.) Trophozoites this large will always divide, forming early schizonts, with two or more segments. Fine, granular, brownish pigment may be abundant. 3. OBJECTIVELY IDENTIFY P. malariae BY EXCLUSION OF P. falciparum and P. vivax. Developing trophozites that extend to the borders of the erythrocyte membrane in bridging “bands” Infected erythrocytes are NEITHER enlarged nor pale and infection typically occurs in older erythrocytes. Schuffner’s dots are absent. Schizonts with no more than 6 -12 segments forming a “rosette” are present. Malarial pigment is abundant and more coarse or “chunky” than that in P. vivax. Gametocytes are present within normalsized erythrocytes. Schuffner’s dots are absent. Aggregates of coarse dark brown-staining malarial pigment may be present. Koneman, Elmer W.; Color Atlas and Textbook of Diagnostic Microbiology, Fifth Edition, Lippencott-Raven Publishers; 1997; page 1126 106731517 SMILE Blood Parasite Smear-Giemsa Stain Appendix 6 Identification Characteristics of Plasmodium Species. CLSI 2004 M15-A Vol. 20:12, pg. 21 Table 1 106731517 SMILE Blood Parasite Smear-Giemsa Stain Appendix 7 Plasmodium Erythrocytic Stages 106731517 SMILE Blood Parasite Smear-Giemsa Stain 106731517 SMILE Blood Parasite Smear-Giemsa Stain 106731517 SMILE Blood Parasite Smear-Giemsa Stain 106731517 SMILE Blood Parasite Smear-Giemsa Stain Appendix 8 Morphological Characteristics of Plasmodium falciparum and Babesia species CLSI 2004 M15-A Vol. 20:12, pg. 24 Table 3 106731517