notes
advertisement

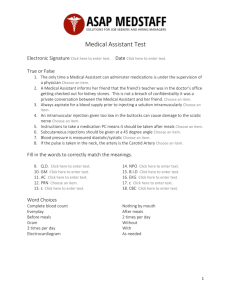
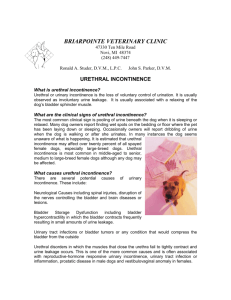
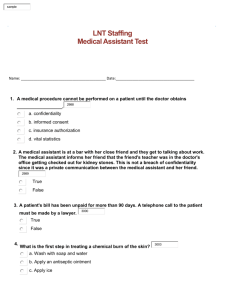
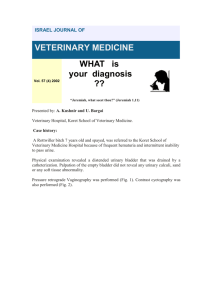
NORMAL AND ABNORMAL MICTURITION Stephen P. DiBartola, DVM LEARNING OBJECTIVES 1. The student will understand the neurologic control of normal micturition including the roles of the parasympathetic, sympathetic and somatic nervous system. 2. The student will understand the difference between neurogenic and non-neurogenic incontinence. 3. The student will understand the difference between an upper motor neuron (UMN or automatic) and lower motor neuron (LMN or autonomous) bladder. 4. The student will be familiar with the most common causes of non-neurogenic urinary incontinence. 5. The student will be familiar with how to take a history and perform a physical examination in an animal with urinary incontinence. 6. The student will understand the diagnosis and treatment of primary sphincter mechanism incompetence. 7. The student will understand the pathophysiology and treatment of reflex dyssynergy. The terms urination and micturition both refer to the passage of urine, but the neurologic integration of urination involves a filling phase as well as an emptying phase. The term urinary incontinence is defined as the loss of voluntary control of urination. In the continent animal, intraurethral pressure exceeds intravesical pressure. If the reverse occurs, the animal becomes incontinent. ABBREVIATIONS FPL = GP = GSE = GVA = GVE = LMN = MUCP = MUP = PPA = UMN = UPP = functional profile length general proprioceptive general somatic efferent general visceral afferent general visceral efferent lower motor neuron maximum urethral closure pressure maximum urethral pressure phenylpropanolamine upper motor neuron urethral pressure profile I. Normal physiology of urination (see Figures 1-3) A. Stretch receptors in the bladder carry afferent information (GVA, GP) about bladder distension to the spinal cord. B. This information is relayed to higher CNS centers (e.g. brainstem, cerebral cortex) via the spinothalamic tract and fasciculus gracilis allowing conscious perception of bladder distension. C. If the circumstances are appropriate for urination, the emptying phase is initiated. The parasympathetic portion of the autonomic nervous system plays the dominant role in the emptying phase. 1. Motor information descends from the higher CNS centers via the tectospinal and reticulospinal tracts to parasympathetic GVE lower motor neurons in the grey matter of the sacral spinal cord (S1-S2). 2. These neurons reach the detrusor muscle of the bladder via the pelvic nerve and initiate detrusor contraction and bladder emptying. 3. This control is mediated by the parasympathetic nervous system and neurotransmission is cholinergic at both the pre-ganglionic and postganglionic fibers. The receptors at the smooth muscle of the detrusor are muscarinic. 4. The GVA and GP afferent neurons from the bladder wall also synapse on the parasympathetic GVE lower motor neurons in the sacral spinal cord. This is the basis for local spinal cord reflex voiding (see below). 5. At the same time, efferent fibers from higher centers inhibit transmission in the sympathetic nervous system, which normally facilitates bladder filling. 6. Also, there is inhibition of GSE neurons located in the sacral spinal cord (S1S3) that exit in the pudendal nerve and normally maintain tone in the striated muscle of the urethra (so-called "external" urethral sphincter). Failure of this inhibition contributes to increased urethral sphincter tone in patients with upper motor neuron bladders. 7. GSE neurons to the striated muscle of the abdomen are stimulated and initiate abdominal wall contractions that increase intra-abdominal pressure and are important in the voiding response. This somatic component represents part of the voluntary control of urination. 8. Injury that results in a CNS lesion cranial to the sacral spinal cord is associated with detrusor areflexia and increased urethral sphincter tone (due in part to loss of UMN inhibitory influence). This results in loss of voluntary control, but manual expression of the bladder is difficult. Within a few weeks of injury, local reflex voiding develops and is associated with incomplete bladder emptying and abnormally high residual volume. Such a bladder is called an upper motor neuron (UMN or automatic) bladder. 2 Figure One: Role of Parasympathetic Nervous System in Urination D. If the circumstances are inappropriate for urination, the filling phase continues. The sympathetic portion of the autonomic nervous system plays the dominant role in the filling phase. 1. Efferent fibers descending from higher centers in the CNS inhibit the GVE lower motor neurons of the parasympathetic nervous system that are located in the sacral spinal cord (S1-S2). 2. Sympathetic GVE in the lumbar spinal cord (L2-L5) are stimulated and these pre-ganglionic fibers synapse at the caudal mesenteric ganglion (cholinergic mediation). The post-ganglionic adrenergic fibers reach the bladder wall via the hypogastric nerve. 3. The post-ganglionic fibers that reach the body of the bladder terminate primarily on beta-adrenergic receptors. When these receptors are stimulated there is relaxation of the detrusor smooth muscle and bladder filling is facilitated. 4. The post-ganglionic fibers that reach the bladder neck and proximal urethra terminate mainly on alpha-adrenergic receptors. When these receptors are stimulated contraction of smooth muscle in these regions occurs which facilitates bladder filling and maintains continence. The smooth muscle in the proximal urethra is referred to as the "internal" urethral sphincter. 5. It is important to recognize that it is the distribution of beta- and alphaadrenergic receptors in the bladder and proximal urethra that determines the role of the sympathetic nervous system in the regulation of urination. 6. Also during bladder filling, efferents descending from higher CNS centers stimulate GSE neurons of the sacral spinal cord (S1-S3) that travel in the pudendal nerve to innervate the striated muscle of the urethra, the so-called "external" urethral sphincter. Neurotransmission at this striated muscle is 3 cholinergic via nicotinic receptors. This somatic component represents part of the voluntary control of urination. 7. Simultaneously, GSE fibers that innervate the striated muscles of the abdomen are inhibited by higher CNS centers. Figure Two: Role of Sympathetic Nervous System in Urination Figure Three: Role of Somatic Nervous System in Urination E. In summary, afferent information from the bladder about its state of distension ultimately reaches higher CNS centers in the brainstem and cerebral cortex. The 4 higher CNS centers integrate this information with other afferent input and institute the appropriate efferent response with respect to urination. F. It is important to understand how the GVE neurons of the parasympathetic and sympathetic components of the autonomic nervous system and the GSE neurons of the somatic nervous system interact in the control of bladder filling and emptying because the drugs that are used to manage animals with disorders of urination act on these systems. G. Even a bladder that has lost its local sacral reflex arc consisting of the GVA and GVE parasympathetic neurons in the sacral spinal cord and pelvic nerve eventually can develop the ability to empty partially. This effect is due to the intrinsic ability of smooth muscle to contract. Urine overflow will occur when intravesical pressure exceeds the elasticity of the urethra. Such a bladder is called a lower motor neuron (LMN or autonomous) bladder and results from lesions in the sacral spinal cord, cauda equina, or pelvic nerves. The residual volume of urine in a LMN bladder usually exceeds that in an UMN bladder. Increasing the animal's intra-abdominal pressure by picking it up may initiate “voiding.” H. Nerves to remember 1. Pelvic nerve (S1-S2) a. Motor to smooth muscle and glands of the pelvic cavity b. Stimulation results in urination, defecation, and erection in the male c. Sensory to the pelvic viscera 2. Pudendal nerve (S1-S3) a. Motor to the external anal sphincter and striated muscle of the urethra, penis, and vulva b. Sensory to the anus, penis, scrotum, clitoris, and vulva II. Abnormal urination (disorders of urination) A. Non-neurogenic 1. Hormone-responsive urinary incontinence. It is unclear how this category of urinary incontinence differs from sphincter mechanism incompetence - the two disorders may be overlapping syndromes or the same syndrome. a. Estrogen-responsive incontinence in female dogs b. Testosterone-responsive incontinence in male dogs (rare) 2. Anatomic abnormality a. Ectopic ureter is most common anatomic abnormality causing urinary incontinence in dogs and cats 5 i. Young at presentation (< 1 year of age; females tend to be presented at a younger age than males) ii. Females affected more often than males iii. More common in certain breeds (e.g. Siberian huskies, Labrador retrievers, Golden retrievers) iv. Ectopic ureter may terminate in vagina or distal urethra v. Unilateral (approximately 67%) or bilateral (approximately 33%) with no predilection for the right or left side vi. Usually diagnosed by excretory urography or ultrasonography vii. Urethrocystoscopy may be the “gold” standard for diagnosis (visualization of both ureteral openings in their normal position conclusively rules out ectopic ureter and abnormal ureteral openings frequently are detected) viii. Often accompanied by other abnormalities (A) (B) (C) (D) (E) (F) ix. x. Hydroureter Hydronephrosis Urethral sphincter mechanism incompetence Bladder hypoplasia Pyelonephritis Renal hypoplasia (uncommon) Surgery is helpful in controlling incontinence in only approximately 50% of affected dogs The owner must be warned that many affected dogs have coexisting urethral sphincter mechanism incompetence and may remain incontinent after surgical correction b. Many dogs with vestibulovaginal stenosis also have urinary incontinence but vestibulovaginal stenosis occurs with similar frequency in continent dogs and this anatomic abnormality is not thought to play a causative role in development of incontinence c. Other anatomic abnormalities associated with urinary incontinence in dogs and cats are rare (e.g. patent urachus, bladder exstrophy, urethrorectal and urethrovaginal fistulas, ureterovaginal fistula after spaying, female pseudohermaphroditism, urethral diverticulum) 3. Paradoxical (obstructive) incontinence (overflow incontinence occurs when intravesical pressure exceeds urethral tone). 4. Incontinence has been reported after prostatectomy in male dogs with prostatic disease 5. Idiopathic incontinence in FeLV-positive cats 6. Incontinence after perineal urethrostomy in cats 7. Urge incontinence associated with urinary tract infection (a form of detrusor hyperactivity or "spastic bladder") 6 8. Idiopathic detrusor hyperactivity (involuntary smooth muscle contractions during the filling phase) 9. Primary sphincter incompetence is the most common non-neurogenic cause of urinary incontinence in dogs a. Common in large breed spayed female dogs (especially Dobermans) b. Maximum urethral closing pressure (MUCP) is significantly lower and functional profile length (FPL) significantly shorter on UPP in affected female dogs as compared to continent female dogs. [See later for explanation of UPP measurements] c. Radiographically, the bladder neck is more caudally positioned (often in the pelvis) in dogs with sphincter mechanism incompetence as compared to continent female dogs. d. Intra-abdominal pressure increases when dogs lie on their sides and this factor may explain why many affected dogs have incontinence while sleeping (i.e. increased intra-abdominal pressure cannot transmitted to the bladder neck and proximal urethra if they lie outside the abdominal cavity in pelvic canal as is the case in many affected dogs). Another contributing factor may be increased parasympathetic (relative to sympathetic) nervous activity while sleeping. e. Most (90%) affected female dogs respond well to PPA alone or to a combination of PPA and estrogen. Estrogens alone are less effective (approximately 60% of affected dogs respond to estrogens alone). f. Refractory cases can be treated by urethral collagen injections under cystoscopic guidance g. Surgical colposuspension immediately improves functional profile length (FPL) and maximum urethral closure pressure (MUCP) postoperatively. It also facilitates transmission of intra-abdominal pressure to the bladder neck and proximal urethra because these structures are pulled cranial and into the abdominal cavity by this procedure. Unfortunately, colposuspension had poor success in a recent study when evaluated one year after surgery. Medical treatment with PPA improved continence in dogs that relapse after colposuspension. h. Sphincter mechanism incontinence occurs rarely in male dogs and is poorly responsive to medical therapy B. Neurogenic 1. upper motor neuron (UMN or automatic bladder) a. b. c. d. e. lesion cranial to S1-S3 partial voiding (intact local reflex arc) high residual volume difficult to express (external urethral sphincter lacks UMN inhibition) loss of voluntary control 7 2. lower motor neuron (LMN or autonomous) a. lesion interrupting local reflex arc (S1-S3) b. partial emptying when intravesical or intra-abdominal pressure exceeds elasticity of urethra c. residual volume usually higher than in UMN bladder d. easy to manually express e. loss of voluntary control 3. Reflex dyssynergy a. Reflex dyssynergy (or dyssynergia) occurs when detrusor contraction is not synchronized with urethral relaxation (i.e. the detrusor contracts but the urethra fails to relax). b. The diagnosis is made by excluding mechanical obstruction (e.g. radiographic studies, passing a urethral catheter) and by observation of urination. Dogs with reflex dyssynergy initiate urination normally but then urine flow stops abruptly and is followed by dribbling c. After observing the dog attempt to urinate, passage of a urinary catheter demonstrates lack of mechanical obstruction and high residual urine volume. Normal residual volume is < 0.4 ml/kg. d. Middle-aged large to giant breed male dogs typically are affected e. Initial treatment traditionally has been to use the non-specific alpha blocker phenoxybenzamine followed by bethanecol in a few days if impaired bladder contractility is suspected. f. Intermittent catheterization to maintain low residual volume and encourage recovery of bladder contractility is recommended during the first few days of therapy. g. Specific alpha-2 blockers have little effect on canine urethral tone and specific alpha-1 blockers may be preferable to non-specific alpha blockers. The specific alpha-1 blocker prazosin may be used at a dosage of 0.1 mg/kg/day divided q8h. The main adverse effect of prazosin is hypotension. h. If alpha blockers fail to relax the urethra, striated muscle relaxants such as diazepam and dantrolene can be considered. i. Chronic bladder hyporeflexia and recurrent chronic UTI are long term complications of reflex dyssynergy. Some dogs require intermittent catheterization by owners at home. j. The condition can be frustrating to treat and may lead to euthanasia. k. Usage of drugs in disorders of micturition is discussed in more detail below III. History A. Signalment 8 1. Congenital disorders are recognized in young animals 2. Hormone-responsive incontinence and urethral sphincter incompetence usually occur in middle-aged, medium to large breed female dogs B. Differentiate loss of voluntary control from behavioral changes or recent onset of polyuria and polydipsia C. Question about dysuria or hematuria suggestive of urinary tract infection D. Question about previous trauma or surgery IV. Physical examination A. B. C. D. Observe the perineal region of females for wetness or foul odor Palpate bladder, urethra, and prostate in males Perform a vaginal exam in females Perform a complete neurologic examination to assess the cerebrum and cerebellum, brainstem, and spinal cord. Pay special attention to the local sacral reflex arc: 1. Consider anal tone during rectal exam 2. Bulbocavernosus reflex (manual compression of the bulbus glandis or vulva causes contraction of the rectum via the pudendal nerve) 3. Perineal reflex (pricking or stroking the skin of the perineum causes ventroflexion of the tail and contraction of the anal sphincter) E. Observe the animal urinating F. Pass a urethral catheter to rule out intraluminal obstruction G. Collect and measure residual urine in the bladder after the animal has finished urinating. Residual urine volume should not exceed 0.4 ml/kg body weight. V. Laboratory findings A. B. C. D. E. Urinalysis Urine culture and sensitivity Contrast radiography (rule out anatomic abnormality) Ultrasonography Special studies 1. The cystometrogram is a pressure-volume recording of the bladder's response to filling with fluid or CO2 9 Figure Four: Cystometrogram showing bladder pressure (cm H2O) as the dependent variable (y-axis) and bladder volume (ml) as the independent variable (x-axis). During the T-II phase the bladder accommodates the accumulation of volume by relaxing (no significant increase in pressure). The bladder approaches its maximal capacity during the T-III phase (pressure begins to rise). The detrusor contracts to initiate voiding at the end of the T-III phase (“thresh”). From Oliver JE, Young WO: Air cystometry in dogs under xylazine-induced restraint. Am J Vet Res 34: 1433, 1973. 2. The urethral pressure profile is a pressure tracing of the urethra as a catheter is slowly withdrawn from the bladder at a constant speed. See Gookin 1996 for an excellent review of this subject. Figure Five: An idealized urethral pressure profile (UPP) from a female dog. Maximum urethral closure pressure (MUCP) and functional profile length (FPL) are the 2 most reliable and widely used parameters in assessment of the UPP. See below for more details. From Rosin A, Rosin E, Oliver J: Canine urethral pressure profile. Am J Vet Res 41:1114, 1980. 10 a. Important parameters for UPP evaluation (see Fig. 5 above): i. Maximum urethral pressure (MUP): highest pressure recorded in profile ii. Maximum urethral closure pressure (MUCP): difference between MUP and intravesical pressure iii. Functional profile length (FPL): length of urethra over which urethral pressure exceeds intravesical pressure. b. FPL is the most consistent parameter on the UPP. MUCP is more variable. MUCP occurs in the middle to distal urethra of female dogs and cats and in the post-prostatic urethra of male dogs and cats. (The male urethra is divided into pre-prostatic, prostatic, postprostatic/penile). 3. The above-described tests are confirmatory in urethral sphincter incompetence, detrusor hyporeflexia, and detrusor hyperreflexia but typically are performed under chemical restraint and not during voiding. Consequently, they do not confirm or rule out reflex dyssynergia. 4. Urethrocystoscopy is helpful to evaluate the vagina, urethra, and bladder and to demonstrate abnormal ureteral openings and other anatomic abnormalities. VI. Treatment A. Definitive 1. 2. 3. 4. 5. Neurogenic: correct lesion if possible Anatomic: correct lesion if possible Paradoxical: relieve obstruction Urge: treat urinary tract infection Hormone-responsive a. Diethylstilbestrol (DES) 0.1-1.0 mg PO 3-5 days followed by 1 mg PO q7d. Adverse effects include signs of estrus, perineal alopecia, and bone marrow suppression. b. 20 μg/kg PO q4d or 0.6 mg total dose q4d of Premarin® (conjugated estrogen supplement containing 50-65% sodium estrone sulfate and 2035% sodium equilin sulfate) has been used as a replacement for DES to treat urinary incontinence in some dogs. c. Estrogen enhances the sensitivity of alpha-receptors to alpha-agonists. These dogs also respond to alpha-agonists, which are safer but require a shorter dose interval. Many dogs treated with estrogen for "hormone-responsive" incontinence probably have primary sphincter incompetence. d. Estrogens used together with PPA may be required to control incontinence in some dogs with refractory sphincter mechanism incompetence. 11 e. Older castrated male dogs with incontinence may be treated with testosterone propionate 2.2 mg/kg IM 3 times/wk or testosterone cypionate 5.5 mg/kg IM q30d. A recent study of males with sphincter mechanism incompetence showed poor (20%) response to testosterone. B. Symptomatic 1. adrenergic agonists a. ephedrine i. ii. iii. iv. adrenergic agent with more alpha than beta effects undesirable effects include tachycardia and CNS stimulation dosage in dogs: 25-100 mg PO q12h to q8h not used very much due to adverse effects b. phenylpropanolamine (PPA) i. alpha adrenergic agent ii. less CNS stimulation than ephedrine and no significant effect on systemic blood pressure iii. dosage: 1.5 mg/kg PO q12h to q8h iv. used for primary sphincter incompetence (helpful in approximately 90% of cases) v. some female dogs with sphincter mechanism incontinence require treatment with both PPA and estrogens to achieve control 2. adrenergic antagonists a. phenoxybenzamine i. ii. iii. iv. nonspecific alpha-adrenergic antagonist adverse effects: hypotension dosage: 0.25 to 0.5 mg/kg q8h or q12h in dogs and cats lowers pre-prostatic urethral tone but has limited to no effect on postprostatic/penile urethral tone in males (i.e. primary effect is on smooth muscle of the urethra) v. used for functional outlet obstruction (e.g. cats with suspected urethral spasm) and to treat reflex dyssynergy in dogs. Reflex dyssynergia initially is treated with phenoxybenzamine. If there is no improvement after 3-5 days, bethanechol (see below) is added b. prazosin i. specific alpha-1 adrenergic antagonist ii. adverse effects: hypotension 12 iii. dosage: 0.1 mg/kg/day divided into equal doses and administered q8h iv. recently has been used to treat reflex dyssynergy in dogs v. contributed to decreased prostatic urethral tone when used along with dantrolene in cats and consequently may have value in management of postobstructive urethral spasm in male cats c. acepromazine i. a phenothiazine with alpha-adrenergic antagonist effects ii. adverse effects: hypotension iii. has been used at a dosage of 0.2 mg/kg SQ q12 or 1.25 mg total dose PO q24h to treat urethral spasm in cats after relief of urethral obstruction. The sedative effect of acepromazine may also be beneficial in this clinical setting. iv. lowers preprostatic and prostatic urethral tone but has no effect on postprostatic/penile tone in male cats 3. smooth muscle stimulants a. bethanechol i. parasympathomimetic agent with primarily muscarinic effects used for detrusor hypoactivity ("bladder atony") or in conjunction with phenoxybenzamine for reflex dyssynergy ii. adverse effects: anorexia, salivation, lacrimation, abdominal cramping, vomiting, diarrhea. Mild nicotinic effect may cause norepinephrine release at sympathetic postganglionic terminals and result in increased urethral tone. Phenoxybenzamine will block this effect. iii. dosage: dogs: 5-15 mg PO q8h; cats: 1.25-5 mg PO q8h 4. other smooth muscle relaxants (e.g. propantheline, oxybutynin, flavoxate, dicyclomine) are used occasionally for suspected detrusor hyperactivity 5. skeletal muscle relaxants a. diazepam i. used for urethral striated muscle spasm ii. dosage: dog: 2-10 mg PO q8h; cat: 1-2 mg PO q8h iii. reports of idiosyncratic hepatotoxicosis in cats treated orally with diazepam suggest that it be used cautiously if at all to manipulate urethral tone in cats iv. furthermore, in one study had diazepam had no discernable effect on prostatic or postprostatic/penile urethral tone in male cats! b. dantrolene 13 i. direct-acting skeletal muscle relaxant used for urethral striated muscle spasm ii. adverse effect: hepatotoxicity iii. dosage: dogs: 1-5 mg/kg PO q12h to q8h iv. decreases prostatic and postprostatic/penile urethral tone in cats REFERENCES 1. Arnold S, Hubler M, Lott-Stolz G, et al. Treatment of urinary incontinence in bitches by endoscopic injection of glutaraldehyde cross-linked collagen. J Small Anim Pract 1996;37:163-8. 2. Aaron A, Eggleton K, Power C, et al. Urethral sphincter mechanism incompetence in male dogs: a retrospective analysis of 54 cases. Vet Rec 1996;139:542-6. 3. Diaz Espineira MM, Viehoff FW, Nickel RF. Idiopathic detrusor-urethral dyssynergia in dogs: a retrospective analysis of 22 cases. J Small Anim Pract 1998;39:264-70. 4. Gookin JL, Stone EA, Sharp NJ: Urinary incontinence in dogs and cats. Part 1. Urethral Pressure Profilometry. Comp Cont Ed Pract Vet 18:407-418, 1996. 5. Holt PE. Long-term evaluation of colposuspension in the treatment of urinary incontinence due to incompetence of the urethral sphincter mechanism in the bitch. Vet Rec 1990;127:537-542. 6. Labato MA. Micturition Disorders. In Birchard SJ, Sherding RG: Manual of Small Animal Practice, Philadelphia: W.B. Saunders Co, 1994, pp 857-864. 7. Rawlings C, Barsanti JA, Mahaffey MB, et al. Evaluation of colposuspension for treatment of incontinence in spayed female dogs. J Am Vet Med Assoc 2001;219:770-5. 8. Richter KP, Ling GV. Clinical response and urethral pressure profile changes after phenylpropanolamine in dogs with primary sphincter incompetence. J Am Vet Med Assoc 1985;187:605-11. STUDY QUESTIONS 1. Describe the sympathetic innervation of the bladder and urethra with special attention to how this innervation facilitates filling and maintains continence. 2. Describe the parasympathetic innervation of the bladder and urethra with special attention to how this innervation facilitates emptying of the bladder. 3. Explain the complementary role of alpha and beta adrenergic receptors in the control of urination. 4. Describe the role of the somatic nervous system in both the filling and emptying phases of urination. 5. What nerve innervates the detrusor muscle of the bladder? The "external" urethral sphincter (the striated muscle of the urethra)? The "internal" urethral sphincter (the smooth muscle of the urethra)? 6. Define urinary incontinence. 14 7. Explain how you would differentiate urinary incontinence from polyuria or dysuria while taking a history from a client. 8. How does an UMN bladder differ from a LMN bladder in cause and clinical management? 9. What type of neurogenic bladder would likely occur in a Dachshund with intervertebral disk protrusion at the T13-L1 interspace? 10. What type of neurogenic bladder would likely occur in a cat with severely displaced sacral fractures? 11. Explain the rationale for the use of urecholine and phenoxybenzamine in the management of reflex dyssynergy. Which drug would you started first and why? 12. How is primary sphincter mechanism incompetence treated? 13. What are the potential side effects of diethylstilbestrol in the treatment of suspected hormone-responsive urinary incontinence? Revised: January 11, 2002 15