BLOOD PRESSURE MEASUREMENT TECHNIQUE IN CHILDREN
advertisement

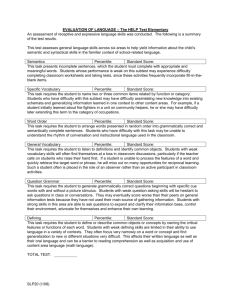
BLOOD PRESSURE MEASUREMENT TECHNIQUE IN CHILDREN Blood pressure should be measured by mercury sphygomanometers, while aneroid sphygmomanometers requires to be calibrated periodically. Automatic osilometric is a good blood pressure measurement instrument for infant and children, because auscultation technique at rest time is difficult to measure in this age group. However, this instrument is quite expensive, needs maintenance, and should be calibrated periodically. The lenght of the cuff bladder should cover at least 80% of the upper arm circumference, and the width of the cuff bladder at least 40 - 75% of upper arm circumference (at a point midway between the olecranon and acromion, see figure 1). An oversized cuff can underestimate the blood pressure, whereas an undersized cuff can overestimate the measurement. Figure 1 Upper arm circumference should be measured midway between the olecranon and acromial process Adapted from Gulati Blood pressure should be measured in a controlled environment after five minutes of rest in the seated position with the right arm supported at heart level. If the blood pressure is greater than 90th percentile, the blood pressure should be repeated twice at the same office visit to test the validity of the reading. Ambulatory blood pressure monitoring (APBM) requires a patient to wear a portable monitor that records blood pressure over a spesific period. APBM usually used in hipertension episodic, chronic kidney failure, hesitant hipertension in adolescent, and in determining the suspicion of organ target injury due to hipertension. Sistolic blood pressure is determined at the time when first Korotkoff sound heard. Diastolic blood pressure is actually heard when the sound insignificant to disappear. Palpation technique is used to measure blood pressure quickly. However, this technique usually reveal 10 mmHg lower than auscultation technique. Limitation Based on The Fourth Report on the Diagnosis, Evaluation, and Treatment of High Blood Pressure in Children and Adolescent : - Hypertension is a sistolic blood pressure and diastolic blood pressure greater than or equal to 95th percentile based on sex, age, and height in three times or more measurement. - Prehypertension is a sistolic blood pressure and diastolic blood pressure greater than or equal to 90th percentile but less than 95th percentile. Look for any risk factor such as obesity. Researches shows that this group has a greater possibility to develop hypertension in adult compared to those in normotension children. - Blood pressure levels greater than or equal to 120/80 mmHg for adolescent must be considered as prehypertension. - Children with blood pressure measurement levels greater to 95th percentile in a medical setting, but normal outside the medical setting called as white coat hypertension. This group has a better prognosis to develop hypertension or cardiovascular disease in later life compared to those with sustain hypertension. - Emergency hypertension is a severe hypertension with life threatening complication such as encephalopathy (stroke, seizure, focal defisit), acute myocard infark, pulmonary oedema, aneurisma aorta, or acute kidney failure. Table 1 shows hypertension classification for children above 1 year of age and adolescent. Blood pressure based on age, sex, and height shows in appendix 1, 2 and 3. Table 1 Hypertension classification in children ≥ 1 year of age and adolescent Classification Normal blood pressure Prehypertension Hypertension Stage 1 hypertension Stage 2 hypertension Limitation Systolic and dyastolic blood pressure less than 90th percentile Systolic or dyastolic blood pressure greater than or equal to 90th percentile but less than 95th percentile Systolic or dyastolic blood pressure greater than or equal to 95th percentile plus 5mmHg Systolic or dyastolic blood pressure from 95th percentile to 99th percentile plus 5 mmHg Systolic or dyastolic blood pressure greater than 99th percentile plus 5 mmHg Evaluation After hypertension been diagnosed, than requires careful anamnesis and physical examination to detect underlying causes and target organ injury. Accurate information by anamnesis and physical examination could avoid evpensive and unecessary laboratory and radiology examination. The evaluation of any hypertension evidence based on age, the degree of hypertension, any organ target injury, and risk factors individually. Appendix 1 Blood pressure levels for boys by age and height percentile Adapted from The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescent Appendix 2 Blood pressure levels for girls by height and age percentile Adapted from The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescent LEARNING GUIDE FOR BLOOD PRESSURE MEASUREMENT BY AUSCULTATION TECHNIQUE STEPS NO. I. Preparation A. B. C. Instrument : 1. Fitting the size of the cuff bladder to the children 2. Choosing the appropriate cuff bladder based on the lenght and the width. The width of the cuff bladder should cover at least 40% - 75% of upper arm circumference at the point midway between the olecranon and acromion. The lenght of the cuff bladder should cover 80-100% of upper arm circumference. 3. Checking the manometers for any mechanic defects that will influenced the measurement: Check for bubble in mercury gauge Turn on the mercury gauge Flow the cuff PLACE : In a controlled situation PATIENT : 1. Not consuming any stimulant drugs or foods 2. Sitting for 5 minutes in a chair with assistance, the leg hang up, and right arm support in a position with the right arm supported at heart level. In younger children, measurement done in a lie down position with arm side straight to the body. II. Blood Pressure Measurement 1. 2. 3 4. Covering upper arm with cuff bladder strongly ± 3 cm from elbow/cubiti fossa as under limit. Determining brachialis arteri position by palpating cubiti fossa then put the stethoscope on it. Pump up the cuff for about 20-30 mmHg above the pressure needs to make occlusion in brachialis artery. Blood pressure the slowly decrease 2-3 mmHg/ secon until korotkoff sound is heard (phase 1 korotkoff = systolic blood pressure), then heard phase-2, phase 3, phase-4 and phase-5. The disappearance of the sound (phase-5) is indicated dyastolic blood pressure (the sound heard quietly), used as a marker of dyastolic blood pressure. After you got the result, map the blood pressure based on Percentile of Height of the children. Determine the diagnosis of the child, is it Normal or Hypertension stage 1 or Hypertension stage 2 SCORE LEVEL 0 1 2