Supplemental Surgical Methods Body Wall Implantation Dogs
advertisement

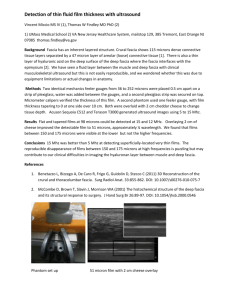
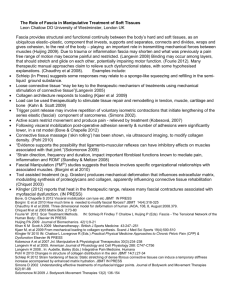
Supplemental Surgical Methods Body Wall Implantation Dogs underwent bilateral body wall implantation of fascia grafts. The dogs were positioned to dorsal recumbency and via a single 10-12 cm ventral abdominal midline incision, skin flaps were developed to expose 3-4 cm on either side of the linea alba in the upper abdomen. 10 x 25 mm portions of the rectus sheath were resected bilaterally in proximity to the umbilicus and approximately 1cm on either side of the midline. The underlying rectus muscle, transversalis fascia, and peritoneum remained intact. A water treated (H20-BW) or THA treated (THA-BW) fascia graft was secured into each defect using 2-0 Prolene (Ethicon Endo-Surgery) simple sutures on the closed end of the stitched loop caudally and the free ends of the stitched fiber in a simple suture configuration cranially (Figure 1B). The skin incision was closed by subcutaneous running 4-0 Vicryl suture. Shoulder Implantation Dogs underwent bilateral shoulder surgery to implant water treated (H20-SH) or THA treated (THA-SH) fascia grafts. The dogs were placed in lateral recumbency, and the infraspinatus tendon was approached and isolated with a 3 cm transverse incision. The infraspinatus tendon was then gently retracted so that the joint capsule under it could be resected to model an open intraarticular injury (Figure 1C). The joint capsule was sharply detached and excised from the inferior edge of the supraspinatus to the superior edge of the teres minor, and from the humeral to glenoid insertions [1]. Care was taken to confirm the absence of bleeding along the cut edges of the capsular injury. The infraspinatus tendon was neither released from its humeral insertion nor otherwise injured [2]. Next, a 5.0 mm Fastin RC anchor (DePuy-Mitek; Rahynam, MA), double-loaded with 2-0 polypropylene fiber (Proxy Biomedical Ltd., Galway, Ireland) was placed in the humeral head approximately one centimeter lateral to the infraspinatus insertion. A fascia graft was laid over the bursal surface of the infraspinatus tendon, insertion site, and bone. With the shoulder in neutral rotation and abduction and approximately 20 degrees of flexion, the fascia graft was first tied down to the anchor with 2 simple sutures through the closed end of the stitched loop. With the graft taut but not further tensioned, it was then attached medially to the infraspinatus tendon using the free ends of the stitched fiber in a criss-cross simple suture configuration (Figure 1D). The wound was then irrigated with normal saline and closed in layers with 4-0 Vicryl suture (Ethicon Endo-Surgery, Blue Ash, OH). The identical procedure was performed on the contralateral limb, except a fascia graft from the alternate treatment group was implanted. References: [1] Derwin KA, Codsi MJ, Milks RA, Baker AR, McCarron JA, Iannotti JP. Rotator cuff repair augmentation in a canine model with use of a woven poly-L-lactide device. J Bone Joint Surg Am 2009;91:1159-71. [2] Van Kampen C, Arnoczky S, Parks P, Hackett E, Ruehlman D, Turner A, et al. Tissueengineered augmentation of a rotator cuff tendon using a reconstituted collagen scaffold: a histological evaluation in sheep. Muscles, ligaments and tendons journal 2013;3:229-35.