Ticket to Work IWP
advertisement

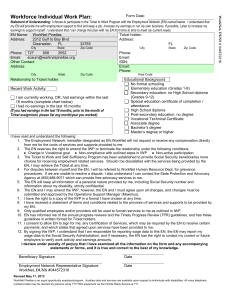
Individual Work Plan PART I Method of completion: (check all that apply) Face to Face by Phone Type of Business Model: (please check one) Employer EN Consumer-Directed Traditional Other (describe) Employment Network (EN) Name: DUNS: EN Address: EN Email: EN Phone Number: Toll Free: Statement of Understanding I choose to participate in the Ticket to Work program with the Employment Network (EN) named above. My participation is VOLUNTARY. I understand that my EN will provide me with continuing employment support to find and keep a job, increase my earnings or run my own business. My plan is to increase my earnings to support myself and achieve self- sufficiency by establishing employment goals that are clear and measurable. I understand that I can change this plan with my EN from time to time to meet my current needs as I work to achieve earnings to support myself. Beneficiary Name: Mobile: SSN: Email: Telephone: Address: The best way to contact me is: (please check one) Email Telephone Mobile Alternate Contact Information Name: Phone Number: Relationship: Address: Email: PARTNERSHIP PLUS (seamless transfer of services) Date of VR closeout ___________ EN assignment Date: __________________ Date of Employment________________________ Beneficiary Employer and Location: _______________________________________ Part II: Employment Goals Name of the VR Agency and VR Counselor: ____________________________ Part II Employment Goals If this is a Partnership Plus Beneficiary continuation, please skip to Part III (Services and Support) after completion of section 1 to continue completion of this IWP. Last Four Social Security Number _______ Page 1 Individual Work Plan Short Term Employment Goals My employment goals and expected earnings Goals to be achieved in 2-24 months (Please note, the acronym S.M.A.R.T are goals that are: Specific, Measurable, Achievable, Realistic and Timely) (RFQ; Sec.3.a.2) Expected Monthly Earnings Hourly or Salary (Should be at or above TWL) 0-$750 $751-$1039 $1040-$2000 $2001-$3500 $3501and above Long Term Employment Goals My employment goals and expected earnings (3 to 5 years) Long Term Goals (Please note, the acronym S.M.A.R.T are goals that are: Specific, Measurable, Achievable, Realistic and Timely) (RFQ; Sec.3. a.2) Expected Monthly Earnings Hourly or Salary (Should be at or above SGA) $1040-$2000 $2001-$3500 $3501and above Part III: Services and Support (The EN agrees to provide these services to help me reach and continue my Employment Goals) My EN and I have agreed upon the supports and services written below. These are the progressive steps the two of us have agreed on to help me reach my employment goals. This includes any referrals my EN agreed to make to help me get services. Career Planning and Guidance (required during IWP development) Services Provided by: Duration of Planning and Guidance 1. (During IWP development) Job search or placement service (required if not working) 2. Services Provided by: 3. Projected Start Date: Job coaching and training (if needed) Services Provided by: 4. Projected Start Date: Job accommodation planning (if needed) Accommodations Required: Last Four Social Security Number _______ Page 2 Individual Work Plan How will my job accommodations needs and outcomes be met? 5. Continuing Employment Supports to assist me in staying employed or to get a better job or higher wages (at a minimum, quarterly contact by EN to assess needs) Projected dates of quarterly contact (Minimum Requirement) Expected Follow up Date of Contact Duration of Contact Name of EN Representative How will my continuing employment needs be met: 1. 2. 3. 6. Other Services: (Referral to other services) (if needed) ** Additional Work Incentives are intended to provide you, (the beneficiary) with the assistance you need to move from benefit dependency to financial independence. Work Incentives help you enter, re-enter or stay in the workforce by protecting your eligibility for cash payments and /or healthcare until you achieve this goal. For more information on work incentives please go to: www.socialsecurity.gov/redbook Part IV: Recent Work History (Check all that apply) * (NOTE: The EN can use the 18 Month lookback form found at https://yourtickettowork.com/web/ttw/en-forms) The lookback form is not mandatory; however, documentation of the last 6 months history is mandatory.) I am currently working. I had no earnings in the last 18 months. I had some earnings in the last 18 months None of my earnings were in the last 6 months Some of my earnings were in the last 6 months Last Four Social Security Number _______ Page 3 Individual Work Plan Employer Start date End Date Wages per hour Hours worked per week Part V: Conditions Related to the Success of my IWP The EN shall discuss with the beneficiary the goals of the Ticket program relative to the beneficiary’s employment, benefits and self-sufficiency so that the beneficiary can make informed choices regarding program participation. The EN has explained the following to me: My participation in the Ticket program is voluntary. It is important that I understand the program’s goals before deciding whether it is right for me. The purpose of the Ticket program is to offer me the support I need to increase my ability to work, my earnings, and the chance that I will become and stay self- supporting to the extent possible. By agreeing to assign my Ticket and participate in the program, I am agreeing to make a steady effort to achieve these aims. The EN’s role is to do all they can to help me reduce and ultimately eliminate my dependency on disability benefits and to earn a better living than I do now. I will not be penalized if I cannot become fully selfsupporting. However, if I decide to use my Ticket, I am making a commitment to try my best to achieve these goals. I can start out working and earning any amount during the first 9 months, but should have a goal to become self-supporting in time. I should work towards having monthly earnings at or above the Trial Work Level (TWL) amount by at least the 10th month after I start working. Also, I should work towards having monthly earnings at or above the Substantial Gainful Activity (SGA) amount a month following my first year of work. The Ticket program is not right for every beneficiary, but if you are committed to trying to become employed and financially independent some day, we are here to provide you the services and support to help you to do so. I will inform my EN of changes in my contact information. My EN will contact me as needed to share information and determine any unmet needs (at least quarterly documented contact). I will inform my EN of my earnings. While I am working, my EN will offer to provide me with ongoing employment support to help me keep working or refer me to others who can help me keep working. My EN has my permission to contact my employer to ensure that I am having a successful employment experience. My EN and I have agreed to the other conditions described below (If no other conditions please state “No other conditions”) Last Four Social Security Number _______ Page 4 Individual Work Plan Part VI Rights and Remedies I UNDERSTAND that I have the following rights under the Ticket to Work program. As my EN you: May not request or accept any compensation from me for the costs of services and supports provided to me as an EN. May change this IWP as long as we both agree. Any change to this IWP must be made in writing. Will provide or help me to obtain ongoing employment support, as necessary, designed to help me keep my job. May unassign my Ticket at any time if either of us is not satisfied for any reason. "Unassignment" letter should be submitted to the Program Manager with their Name, SSN, Date, Signature and the name of the EN. Informed me of the Timely Progress Review guidelines. Will keep my personal information, including my Social Security number and information about my disability private and confidential. Will use only qualified employees and/or providers to provide services to me. Will provide me with a copy of this IWP and any changes in an accessible format. May offer services outside of your Ticket services. Should I choose to purchase a service outside the Ticket services, a separate acknowledgment must be signed by both of us and attached to this IWP. Explained your dispute resolution process, if we are unable to resolve a dispute, another process is available to me through the Ticket Call Center at 1-866-968-7842. Part VII: Acknowledgement and Signatures I declare under penalty of perjury that I have examined all the information on the form and any accompanying statements or forms, and it is true and correct to the best of my knowledge. By signing below, (1) I acknowledge assignment of my ticket to this EN; (2) I agree to the terms of this IWP; (3) give permission for the EN named in this IWP to contact employers on my behalf to verify or obtain evidence of work or earnings. Beneficiary Name (Print) ________________________________________________ Beneficiary Signature ______________________________Date_________________ EN Representative Signature ________________________Date_________________ ENs shall maintain a file of all IWPs prepared for Ticket Holders. Social Security reserves the right to request copies of any/all IWPs for audit purposes. Last Four Social Security Number _______ Page 5