Injectable Biomaterials for Augmentation of the Nucleus Pulposus
advertisement

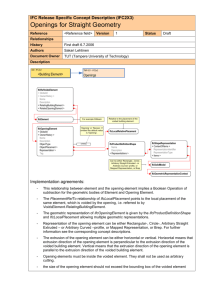
Extrusion Resistance of an Injectable Nucleus Replacement in the Human Cadaver Spine Jared Walkenhorst, M.S.1, Dennis Lee, M.S.1, David Spenciner, Sc.M.2 1 Spine Wave, Inc. Shelton, CT, 2RIH Orthopaedic Foundation, Providence, RI INTRODUCTION: The NuCore Injectable Disc Nucleus (IDN) is an in-situ curing hydrogel intended as an adjunct to discectomy. The IDN replaces excised nuclear tissue and is injected through an annular deficit created during a nucleotomy. Because it interdigitates with the surrounding tissue, it is important to understand how well it is constrained by the surrounding tissue and whether it will remain in place even under high physiologic loading. 5,000 OBJECTIVE: The purpose of this study was to evaluate how well the IDN would resist extrusion from the disc space by testing human cadaveric anterior column units (ACU: a functional spinal unit with posterior elements removed) in compression after injection with IDN. ACUs were tested in the neutral posture. In addition, because some literature indicates that disc herniation is more likely in extreme bending, ACUs were also tested in flexion. 4,500 4,000 Failure Load (N) 3,500 Figure 1: Hyperflexed Extrusion Set-Up 3,000 2,500 2,000 1,500 Compression Flexion Test of 706-T11/T12 with posterior-lateral partial discectomy (8/12/03). Stiffness = 735.0 N/mm. Yielding = 2411.8 N at 5.96 mm. Ultimate Load = 2891.6 N at 7.78 mm. No observed extrusion. 1,000 500 3,500 0 #1 3,000 Results of the hyperflexion testing are shown in Table 2 and Figure 5. In the flexed compression testing of lumbar ACUs, the average load to failure was 2,637 N. The load to failure was lower than neutral testing because the flexion caused narrowing of the anterior disc space resulting in an earlier collapse of the anterior rim. In all eleven cases, failure of the ACU was by endplate fracture, failure of the anterior rim, or cancellous bone failure. No samples failed by extrusion of IDN. In three cases, small volumes (<0.1 mL) of IDN was expulsed through the annulotomy at or after failure of the bone. It is believed the IDN extrusion was caused by disc space collapse brought on by bony failure. In addition, in one case, natural nucleus was expelled through the annulotomy during the test, while IDN remained in place. REFERENCES: 1. Nachemson et al., Acta Orthop Scand, 1963. 2. Nachemson et al., J Bone Joint Surg 1964. 3. Wilke et al., Spine 1999. #4 #5 #6 #7 #8 *#9 #10 Figure 4: Extrusion in Neutral Posture Stiffness Calculated from Linear Regression Initial Yielding 1,500 Toe Region Due to Fixture Rotating into 12 deg Flexion 1,000 5,000 4,500 4,000 500 3,500 0 1.0 2.0 3.0 4.0 5.0 6.0 7.0 8.0 9.0 10.0 3,000 Figure 3: Sectioned Test Specimen. IDN is intact within the disc space Load (N) 0.0 Figure 2: Typical Force-Displacement Curve In the neutral compression testing of lumbar ACUs, the average load to failure was 3,555 N. Results are presented in Table 1 and Figure 4. In all ten cases, failure was by endplate fracture or cancellous bone failure. No samples failed by extrusion of IDN. #3 2,000 Displacement (mm) RESULTS: Each specimen was sectioned after testing to verify presence of the IDN and observe its state. Each section was photographed. As shown in Figure 3, the IDN remained intact and in place up to and after bony failure. In some cases of endplate failure, IDN migrated into the cancellous bed of the vertebral body, but did not extrude through the annulotomy. #2 * IDN extrusion observed well after endplate failure. 2,500 Load (N) METHODS: Each ACU was given a partial nucleotomy (≈1.5mL) through a standard posterior 5 x 5 mm cruciate annulotomy. Each specimen received an injection of IDN such that the material filled the cavity to the inside of the annulotomy. After curing of the IDN, each ACU was subjected to compression testing in a servohydraulic test frame to failure. Ten ACUs were tested in neutral posture, eleven were tested in flexion with the angle oriented in the plane of the annulotomy as shown in Figure 1. The maximum load and failure mode were observed and recorded from Force Displacement Curves as shown in Figure 2. After testing, each specimen was sectioned and examined. Ultimate Load Linear Regression 2,500 2,000 1,500 1,000 500 Table 1: Extrusion Test Results for Neutral Set-Up Sample Extrusion Load (N) Failure Load (N) 634 L2/L3 NONE 3608.8 634 L5/S1 NONE 4701 Failure Type Cancellous Failure Cancellous Failure 635 L1/L2 NONE 2897.6 Endplate Failure 637 L1/L2 NONE 3279.5 637 L3/L4 NONE 4129.1 636 L1/L2 NONE 634 L3/L4 75 L3/L4 Table 2: Extrusion Test Results for Hyperflexion Set-Up Sample Failure Load (N) 673 L3/L4 NONE 2093 Failure Type Central Endplate Failure 688 L1/L2 2751 a NA Anterior Rim Failure 2040 NP Extrusion 688 T11/T12 (2040) Endplate Failure 673 L1/L2 NONE 3093 Cancellous Failure Endplate Failure 709 T12/L1 NONE 2769 Anterior Rim Failure 3717.2 Endplate Failure 706 T11/T12 NONE 2892 Cancellous Failure NONE 3976.5 NONE 2826 Cancellous Failure 3096.4 Endplate Failure Cancellous Failure 706 L2/L3 NONE 706 L3/L4 2611 2651 3154 Endplate Failure 707 L2/L3 NONE 1544 Cancellous Failure Central Endplate Failure 2992.2 Endplate Failure 707 L4/L5 NONE 2139 Cancellous Failure a 75 L1/L2 NONE 532 L1/L2 NONE Average N/A 3555.2 S.D. N/A 581.7 Note a: IDN extrusion through annulotomy observed after 8.5-mm of displacement @ 3100 N. N/A N/A 708 L2/L3 Average S.D. Note a: Note b: NONE 4320 3227 2637 N/A 764 Extrusion of IDN after yielding Extrusion of Natural Nucleus #1 * #2 #3 #4 #5 #6 #7 * #8 #9 #10 #11 * Extrusion of IDN after yielding of ACU ** Extrusion one IDN particle coincident with ultimate failure Extrusion Load (N) b 0 Anterior Rim Failure N/A N/A Figure 5: Extrusion in Hyperflexion Posture DISCUSSION: Literature has predicted the loads through the disc during daily living to be approximately 1200 N.[1][2][3] All tests exceeded this load prior to any failure. The three cases of small IDN extrusion occurred well after 1200 N was reached. To understand what happens after bony failure, some tests were continued after failure was observed. In those tests, the IDN migrated through the fractured endplate and into the cancellous bed. When the disc was sectioned, much of the IDN was no longer in the disc space. It is believed the IDN migration into the vertebra was caused by disc space collapse brought on by bony failure. CONCLUSIONS: The results of this study indicate the IDN was successfully secured by the surrounding tissue within the disc space. Extreme compressive loads did not cause extrusion of the IDN prior to bony failure of the segment. These results indicate the IDN performs well under high physiologic loads.