SELF-ASSESSMENT FORM FOR MALE TNT CLINIC
advertisement

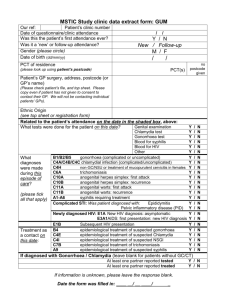
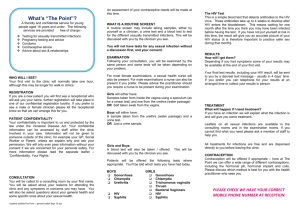
CLINIC LABEL MALE SELF-ASSESSMENT FORM FOR CHECK AND GO NAME ……………………………………………… MY MOBILE NUMBER IS: ………………………………… If you have no symptoms and you just need a check up for peace of mind . Fill out and sign an assessment form and see a nurse. You choose which tests you want A swab test for gonorrhoea and Chlamydia , Blood tests for HIV and Syphilis Results will be by text message –in 2-3 weeks Free condoms, No treatment Tell the receptionist if you feel that this service is not what you require. When did you last pass urine less than 2 hours Have you ever had sex with a man? yes on Have you ever injected drugs? Request for tests: I would like to have the following tests: yes on Swab/urine test for Gonorrhoea yes on Swab/urine test for Chlamydia yes on Blood test for HIV yes on Blood test for Syphilis yes on Consent I confirm that I have read and understood the information form about Gonorrhoea, Chlamydia, HIV and Syphilis testing. I understand that I will not be tested for other condition, have any discussion regarding lifestyle changes or be provided with any contraception other than condoms. I request that the result should be sent by text message. Signature:………………………………………….. Date: …………. To be completed by health care workers Number of 3months 1 year Test partners Male Female Taken Date Sign G.C Chlamydia sts HIV KC60 CODES Nurse signature……………………………………... Date…………..