THE WILLIAM W - Anticoagulation Centers of Excellence
advertisement

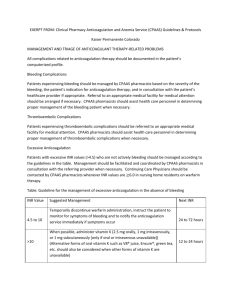
SUBJECT: ANTICOAGULATION CLINIC PROTOCOL PAGE 1 OF 3 DEPARTMENT OF PHARMACY SERVICES EFFECTIVE: 12/96 APPROVED BY: Pharmacy and Therapeutics Committee REVISED: 3/97, 8/98, 1/99, 2/07, 3/08, 2/12 I. GOALS a. The William W. Backus Hospital Anticoagulation Clinic is designed to assist physicians in improving quality of care provided to their patients on anticoagulation therapy. Ultimately, our goal is to assure that these services improve patients' therapeutic outcomes, reduce complications of anticoagulation therapy, and reduce hospitalizations. Specific goals include: i. ii. iii. iv. Improving continuity of care for patients on anticoagulation therapy Providing patient education on disease state and drug therapy Reducing adverse effects of anticoagulation therapy Maximizing the benefits of anticoagulation therapy II. OBJECTIVES a. Provide a monitoring service for physicians initiating and continuing long-term anticoagulation. b. Provide education and routine follow-up for patients including disease state information, monitoring requirements, drug therapy consultation, and drug compliance assessment. c. Reduce adverse effects resulting from warfarin therapy by screening for drug-drug interactions, drugdisease state interactions, drug-food interactions, and for signs and symptoms of unusual bruising or bleeding or embolic events. d. Assist physicians in maximizing the benefits of warfarin therapy by maintaining the patients' INR values within the optimum therapeutic range. e. Coordinate anticoagulation therapy during perioperative periods. III. DESIGN a. The William W. Backus Hospital Anticoagulation Clinic is an outpatient, ambulatory clinic that provides comprehensive care to individuals diagnosed with coagulation disorders and/or receiving anticoagulation drugs. The Clinic utilizes a Point of Care (POC) device to assess the effectiveness of warfarin therapy. Patients are assessed by anticoagulation care providers comprised of advanced trained pharmacists and nurses. A licensed physician oversees the activities of the care providers. An Anticoagulation Clinic Physician will be available for consultation during the hours of operation. IV. PROCEDURE a. Referral i. Individuals will fall under the care of the clinic after a physician involved in the care of the patient completes and forwards an "Anticoagulation Clinic Referral" form. Anticoagulation care by the Clinic commences once the patient has their first clinic visit. Referrals are only accepted for ambulatory patients able and willing to visit the clinic in person. ii. Once received, Referral Forms are immediately reviewed by a Care Provider for appropriateness and completeness and to determine the urgency of the patient’s first visit. Missing information will be promptly obtained from the referring physician. iii. Patients will be contacted as soon as able to schedule their initial visit. iv. Referred patients without a primary care physician (PCP) or other managing physician (MP). 1. All patients being managed by the clinic need to be under the care of a primary care physician or other physician managing the patients care. Patients referred to the clinic that are not under the care of a PCP/managing physician will be managed by the clinic as soon as clinically required, but will be given a limited time period to obtain a primary care physician or appropriate specialist. 2. During the initial visit, PCP information will be obtained. 3. Those not having a PCP/managing physician will be given a list of area Family and Internal Medicine physicians and appropriate specialists and be instructed of this policy and requested to obtain a physician within three months. 4. If after three months the patient still has not obtained a PCP/MP, A certified letter will be sent to the patient to inform them that they have 3 more months to secure a PCP/MP or their anticoagulation therapy will no longer be monitored by the clinic. 5. If after a total of six months, the patient still has not obtained a PCP/MP, a Clinic discharge letter will be sent to the patient to inform them that they will no longer be managed by the clinic. b. Patient’s initial visit i. After reception of a referral form, the patient will be contacted to arrange for their initial visit to take place at the earliest opportunity. During the initial visit, an anticoagulation care provider will review the referral and any additional pertinent medical information. This information will be recorded in the patient’s anticoagulation clinic chart. ii. Patients will be notified of their HIPAA rights and Clinic policies and sign the following forms: (See appendix) 1. Anticoagulation Clinic Consent, Release of Information, Guarantee of Payment Form 2. Clinic Contract with Patient c. Education Session i. Patients will be scheduled for at least one 45-minute educational visit to occur at the earliest opportunity. This session will consist of a multimedia presentation, a focused lecture, and a question and answer section. The education will focus on the risk and benefits of anticoagulation therapy, thromboembolic disorders, and safe medication practices. Information regarding the clinic’s design, working hours, and procedures will also be discussed. Patients may elect to refuse this session as well as repeat it at any time during their care. (See appendix) d. Standard Visit or Encounter i. At each scheduled appointment, the patient will be interviewed and assessed by a care provider (or student being overseen by a care provider) for the following current and potential information: 1. Signs and symptoms of hemorrhagic or embolic complications 2. Changes in dietary or alcohol habits 3. Recent changes in life style or health status 4. Status of medical problem necessitating anticoagulation therapy 5. Changes in medication regimen including OTC and herbal preparations 6. Compliance issues related to medication regimens 7. Confirmation of current anticoagulant regimen ii. The care provider will perform a POC PT/INR test. (See Policy: Whole Blood Prothrombin Time) The result of the test will be compared to the therapeutic range that is prescribed for the patient and their current health status and/or issues discussed as above. For all POC INR results greater than 4, a confirmatory venipuncture PT/INR should be drawn. For all INR results greater or equal to 4.5, the clinic physician must be directly consulted. The care provider will directly evaluate other INR results at the time of visit. The management of the result will depend on the many patient factors obtained above as well as the patient’s individual risk of hemorrhagic or embolic complications (if identifiable). Attachment 1 will be used to guide the management decisions. All appropriate information will be communicated to the patient or designated caregiver. Follow-up appointments will be scheduled before the end of the visit. Follow-up should occur no greater than 4 weeks later, but may occur as early as 24 hours. See Attachment 2 for general guidelines. iii. When there is clinical suspicion of anemia or occult bleeding including but not limited to sample error on POC testing device, new onset or worse than baseline, shortness of breath, pale appearance, or tiredness: A hemoglobin/hematocrit lab test will be ordered as per the Clinic Medical Director and followed up as follows: HGB > 10 HGB 7-9 Copy of lab result forwarded to patients primary care provider Primary care provider notified immediately HGB < 7 Patient immediately referred to the Emergency Department. The patient as well as the Clinic Medical Director will also be informed of all results when available. iv. At the conclusion of the visit, the patient will be given an appointment card with the Clinic’s phone number and date and time of follow-up visit on the front. The back of the card will indicate the patient’s INR result and dosage regimen. e. Care of Patients Unable to Visit the Clinic i. Patients unable to travel to the clinic due to medical or temporary logistical reasons may be cared for through telephone consultations and INR results obtained by other laboratory services. The telephone interview and management process will be of the same procedure listed above for a standard visit. f. Management of Critical Values i. INR results >4.5 or otherwise deemed critical by the care provider need to be communicated to the clinic physician (or patient’s primary care physician) as soon as able. On the direction of a licensed prescriber, a sample dose of oral phytonidione (Vitamin K) may be dispensed to the patient by a licensed prescriber (APRN) or pharmacist with proper labeling and instruction and documented on the “Vitamin K Sample Log”. ii. Any orders given by the clinic physician by telephone or verbal means must be immediately transcribed into the patient’s profile and signed by the physician within 24 hours. g. Perioperative Management i. Patients currently receiving anticoagulation therapy offer unique and difficult therapeutic challenges when needing a percutaneus medical procedure. ii. Patients should be interviewed at each visit for the possibility of planned percutaneous procedures. iii. When a medical procedure is pending, a thromboembolic and hemorrhagic risk assessment should be completed and resulting treatment strategies discussed with the patient (see appendix). When necessary, the patient’s primary care provider, surgeon, dentist, gastroenterologist or other physicians as well as the clinic physician should be consulted for final approval of treatment strategies. h. Documentation i. Patient Profile 1. An electronic patient profile will be maintained in the Meditech system for all active patients. Documentation will include a minimum of: a. Diagnosed reason for anticoagulation b. Other medical conditions c. Contact information d. Current warfarin tablet strength e. Therapeutic range f. Expected duration of anticoagulant treatment g. Referring physician ii. Individual Visit Documentation 1. At each patient visit the following items will be documented in the Meditech PCS system: a. PT/INR results b. Warfarin dosage regimen c. Education topics covered d. Whether the encounter was by telephone or in person e. Relevant clinical information obtained from the patient interview f. Instructions given to the patient g. Date of follow-up appointment (entered in Meditech SCH) h. Billing level iii. Printing and review of Summary Sheets 1. A patient visit summary sheet containing this information as well as the pertinent profile information listed above will be printed for all patient visits that occurred that day. 2. These sheets will be reviewed and signed by the clinic physician within 24 hours. a. The physician’s signature will indicate agreement with the documented treatment plan including dosage recommendation, date of follow-up visit and any patient instructions given. b. If the reviewing physician disagrees with any of the documentation, they may either notify the patient themselves (if medically warranted), or document the changes they want to be implemented and notify the Clinic staff of the changes. c. Any orders given by the clinic physician by telephone or verbal means must be immediately transcribed into the patient’s profile and signed by the physician within 24 hours. i. Prescriptions i. Prescriptions for anticoagulant drugs for clinic patients should originate from the clinic. To reduce the chance of error, telephone prescriptions should only take place when necessary due to time and technological constraints. Prescriptions should be written and given to patients and/or faxed to pharmacies. Prescriptions may be filled out by care providers but must be signed by a licensed prescriber before being telephoned or otherwise transmitted to a pharmacy. j. Billing i. Patients will be billed for the encounter only if all of the following take place: 1. The patient was interviewed and assessed in the clinic by a care provider 2. A PT/INR test was done 3. Education was offered V. Care Providers a. Anticoagulation Care Provides must: i. Be a Connecticut licensed pharmacist, nurse, physician’s assistant or physician. ii. Have completed a basic assessment of knowledge and skills (see appendix). b. Students may interview, assess and instruct patients providing: i. They have completed a basic assessment of knowledge and skills. ii. Assessment and instructions are reviewed by a Care Provider prior to the instructions being given to the patient. iii. All documentation done by the student must be reviewed and co-signed by a care provider before the end of the working day. VI. HIPAA see The William W. Backus Hospital HIPAA Policy and Procedure Manual VII. Quality Assurance a. Quality assurance will be carried out through the following activities: i. Monthly tracking of overall percent of patients within their therapeutic range. ii. Monthly tracking of overall percent of INR results >4.0 iii. Monthly tracking of number of clinic patients admitted for hemorrhagic or thrombotic events. 1. “Peer review” is performed on each identified case. b. Quarterly report of above indicators to the Pharmacy and Therapeutics Committee. Attachment 1 Recommendations for Managing Bleeding or INRs Outside of the Therapeutic Range Condition INR below therapeutic range; no signs of thrombosis Recommendation Increase dose in increments of 5 to 20% based on the cumulative weekly dose or monitor more frequently; a one-time larger dose may be given followed by more frequent monitoring; if only minimally below therapeutic range, no dose increase may be required INR above therapeutic Lower dose in increments of 5 to 20% based on the cumulative weekly range but < 5.0; no dose or omit dose, monitor more frequently, and resume at lower dose significant bleeding when INR therapeutic; if only minimally above therapeutic range, no dose reduction may be required INR 5.0 but < 9.0; no Omit next one or two doses, monitor more frequently and resume at lower significant bleeding dose when INR in therapeutic range. Alternatively, omit dose and give vitamin K1 ( 5 mg orally), particularly if at increased risk of bleeding. If more rapid reversal is required because the patient requires urgent surgery, vitamin K1 (2 to 4 mg orally) can be given with the expectation that a reduction of the INR will occur in 24 h. If the INR is still high, additional vitamin K1 (1 to 2 mg orally) can be given INR 9.0; no significant Hold warfarin therapy and give higher dose of vitamin K1 (5–10 mg orally) bleeding with the expectation that the INR will be reduced substantially in 24–48 h. Monitor more frequently and use additional vitamin K1 if necessary. Resume therapy at lower dose when INR therapeutic Serious bleeding at any Hold warfarin therapy and give vitamin K1 (10 mg by slow IV infusion), elevation of INR supplemented with fresh plasma or prothrombin complex concentrate, depending on the urgency of the situation; recombinant factor VIIa may be considered as alternative to prothrombin complex concentrate; vitamin K1 can be repeated every 12 h Life-threatening bleeding Hold warfarin therapy and give prothrombin complex concentrate supplemented with vitamin K1 (10 mg by slow IV infusion); recombinant factor VIIa may be considered as alternative to prothrombin complex concentrate; repeat if necessary, depending on INR * If continuing warfarin therapy is indicated after high doses of vitamin K1, then heparin or LMWH can be given until the effects of vitamin K1 have been reversed and the patient becomes responsive to warfarin therapy. It should be noted that INR values > 4.5 are less reliable than values in or near the therapeutic range. Thus, these guidelines represent an approximate guide for high INRs. Adapted from: Ansell J et al. The pharmacology and management of the vitamin k antagonists: the seventh ACCP conference on antithrombotic and thrombolytic therapy. Chest 2004;126;204-233 Attachment 2 Recommendations for scheduling of follow-up clinic visits The optimal frequency of long-term INR monitoring is influenced by patient compliance, transient fluctuations in comorbid conditions, the addition or discontinuation of other medications, changes in diet, the quality of dose-adjustment decisions, and whether the patient has demonstrated a stable dose response. In newly treated patients, INR monitoring should be performed daily starting after the second or third dose until the therapeutic range has been achieved and maintained for at least 2 consecutive days, then two or three times weekly for 1 to 2 weeks, then less often, depending on the stability of INR results. When the INR response is stable, the frequency of testing can be reduced to intervals as long as every 4 weeks. If adjustments to the dose are required, then the cycle of more frequent monitoring should be repeated until a stable dose response can again be achieved. Small dosage adjustments (5-10% of weekly dosage) will require patients return for follow-up in one weeks time. Larger dosage adjustments may require the patient to return to daily consecutive visits until dosage stability is regained. As a general rule, patients with 2 consecutive INR’s within the therapeutic range a week or more apart may be seen again in two weeks time. Patients with 3 consecutive INR’s within the therapeutic range 3 weeks or more apart may be seen again in four weeks time. This assume that during this period of time, there has been no change in the patients medical status, medication regimen, or diet. Appendix 1. 2. 3. 4. 5. 6. Anticoagulation Clinic Referral Form Anticoagulation Clinic Consent, Release of Information, Guarantee of Payment Form Contract with Patient Education Guidelines New Patient Orientation Check List Anticoagulation Bridging Protocol The William W. Backus Hospital Anticoagulation Clinic Referral Form/Ambulatory Summary Phone #: (860) 892-2711 Fax#: (860) 425-8791 Patient Name: ______________________________ DOB: ___________ Allergies:__________________________ MRN#: ________ Phone #: _______________ Caregiver/Relative’s name & contact information: __________________________________ Check Appropriate Diagnosis Box and Enter Projected End Date INR Recommended Projected End Check Indication Range Length of Therapy date Stroke Prevention Atrial Fibrillation 2-3 Indefinite Atrial Fibrillation with planned cardioversion 2-3 3wks prior/4wks post Other stroke prevention 2-3 Prosthetic Heart Valve Aortic 2-3 Indefinite Mitral 2.5-3.5 Bilateral Bioprosthetic/tissue valve DVT/PE Treatment and/or Prevention DVT/PE Single event w/transient risk factors DVT/PE Single event no precipitating cause DVT/PE Thrombophilic disorder DVT/PE with Hx of multiple thrombotic events With Cancer (consider LMWH treatment for first 3-6 months) DVT/PE while receiving adequate anticoagulation Post orthopedic surgery prophylaxis 2.5-3.5 2-3 3 months 2-3 2-3 2-3 2-3 2-3 2.5-3.5 2-3 3 months 3 mo- indefinite 6 mo- indefinite Indefinite 1 yr-indefinite Indefinite 10-35 days (Recommendations consistent with the 8th ACCP Consensus Conference on Antithrombotic Therapy) OTHER (please be specific) DX: Range Length of therapy Other instructions: Start date of therapy: Patient is currently on a LMWH Social History: Lives alone PMHx: Peptic Ulcer Disease Renal Insufficiency Pulmonary disease Warfarin tablet strength ______mg Current dosing regimen: Smoker Alcohol use (Alcohol abuse is a contraindication for warfarin therapy) Hypertension Diabetes Mellitus Arthritis Cancer of ________ Thyroid disease Seizures Anemia Heart Failure GI bleeding Mental Health Hx of Falls IV Drug Abuse Hepatic disease Hypercholesteremia Cognitive Impairment Other: ___________________________________________________ Surgical History: Referred patients will be managed according to the Anticoagulation Clinic Protocol Physician: Signature: Primary Care Physician (if different): Date: Time: Place addressograph sticker here Patient Name: ______________________ DOB: ______________ V# ______________ M# ______________ William W. Backus Hospital Anticoagulation Clinic 111 Salem Turnpike Norwich, CT 06360 Contract with Patient I understand that, as a participant in the anticoagulation clinic, I am required to be present at all clinic appointments. I understand that I will call the anticoagulation program if I do not receive instructions within 48 hours after a blood test or if my medical condition (including medicines) changes. I am able to travel to the clinic or arrange for transportation for my appointments. I am willing to follow instructions involving compliance with Warfarin dosage and administration, proper diet, and notifying the clinic regarding all drugs that I am taking (even over-the-counter & herbals). I have access to a telephone and can be reached by telephone if necessary. I am taking a medicine that must be followed closely in order to protect me from any complications. I understand that my noncompliance with any of the above can result in serious health risks and/or termination with the program. ________________________________________ Patient signature ______________ Date ________________________________________ Anticoagulation Clinic staff signature ______________ Date PATIENT EDUCATION Education is one of the most important aspects of successful anticoagulant control. Verbal, written, and audio-visual patient information materials will be individualized and available for each patient (available in foreign languages). The education process should begin with a formal session involving the patient and any care takers or family members that wish to participate. The process of patient education will be continuous and reinforced at every patient encounter. The care provider will work with the patient to enhance their knowledge. If there is difficulty in assessing patient's competence or documentation of non-comprehension, the patient will be referred back to the primary care physician. Topics include, but are not limited to: Indication of medications Understanding of disease state Name, strength, dose, and description of medications Administration times and method of administration How to use medication containers and compliance aids Importance of keeping this medication safely away from children. Importance of medication wallet cards and MedicAlert bracelets Potential drug and food interactions Potential drug and drug interactions Symptoms of embolic event and emergency symptoms Symptoms of unusual bruising and bleeding and emergency symptoms Importance of laboratory monitoring of therapy Importance of compliance with treatment regimen and follow-up visits Importance of notifying clinic staff when changes occur to medication regimen, diet, or health status Importance of notifying clinic staff about planned medical and dental procedures William W. Backus Hospital Anticoagulation Clinic 111 Salem Turnpike Norwich, CT 06360 Patient Name: _______________________ DOB: ______________ M# ______________ New Patient Orientation Checklist INITIAL VISIT: Complete “Initial Visit Patient Encounter” sheet Provide “Patient’s Guide to Using Warfarin Therapy” booklet Sign consent form & clinic contract Clinic hours/Staff What is warfarin & why do I need it? Taking warfarin (how much, when, missed dose) Warfarin tablet identification Common side effects of warfarin What is PT/INR blood test? Signs/symptoms of bleeding/stroke/DVT/PE & actions to take Address patient questions Patient education completed on ___/___/___ by __________________________ SECOND VISIT: Provide “Patient’s Guide to Using Warfarin Therapy” booklet (if needed) What causes INR to change? Drug Interactions Warfarin and Vitamin K in diet Pregnancy “Other things to think of”: Surgical & dental procedures ID/Medic Alert Traveling Prescription renewal info Address patient questions Patient Education Evaluation Quiz Patient education completed on ___/___/___ by __________________________ DVD: “Staying Active and Healthy with Blood Thinners” (optional) Viewed on _______________ Patient Declined ______________ William W. Backus Hospital Anticoagulation Clinic Anticoagulation Bridging Protocol Patient: Physician: DOB: Allergies: Procedure Date: Procedure Type: Clinical trials and expert opinion indicate that oral anticoagulation therapy can be continued without increasing the risk of major bleeding for single and multiple dental extractions, joint and soft tissue injections and arthrocentesis, cataract surgery, and upper endoscopy or colonoscopy with or without biopsy. Supporting data will be supplied if requested. Please carefully consider the effect that stopping warfarin therapy for a few days can have on the patient. A moderate amount of bleeding is a minor inconvenience compared to a paralyzing stroke or death. Thromboembolic Risk Assessment Low Risk Atrial Fibrillation Prosthetic Heart Valve Venous Thromboembolism CHADS2* 0-2 No prior stroke or TIA Valve Bileaflet aortic valve prosthesis without Afib, and no other risk factors for stroke. Bileaflet aortic valve prosthesis and any of the following: atrial fibrillation, prior stroke or TIA , hypertension, diabetes, CHF, age >75 Single VTE event greater than 12 months ago and no other risk factors VTE within past 3-12 months. Recurrent VTE Active cancer (treated within 6 months) Non-severe thrombophilia (heterozygous factor V Leiden mutation, Heterozygous factor II mutation) CHADS2* 5-6 Any mitral valve prosthesis. VTE within 3 months High Risk Stroke or TIA within 3 Caged-ball or tilting disk aortic Severe thrombophilia (protein C, S or months; rheumatic valve prosthesis. Stroke or TIA antithrombin deficiency, antiphospholipids valvular heart disease. within previous six months. antibody, or multiple abnormalities) *CHADS2: 1 point each for presence of CHF, hypertension, Age >75, Diabetes and 2 points for prior stroke or TIA. Intermediate Risk CHADS2* 3-4 Desired bridging strategy (check one): Questions concerning bridging may call Clinic Medical Director, Dr. Jan Akus 886-1494 Low Risk Hold warfarin for 5 days prior to procedure, check INR 1 day prior, If ≥ 1.5 administer 1.25mg Vitamin K PO Resume warfarin the day of procedure. Intermediate/High Risk: Hold warfarin for 5 days prior to procedure; enoxaparin 1.5mg/kg/day when INR is below the patient’s defined therapeutic range. On the day prior to the surgery/procedure, administer 0.75mg/kg. Minor surgery/low bleeding risk: Resume enoxaparin 1.5mg/kg/day 24 hours after the procedure. Moderate bleeding risk: Resume enoxaparin 1.5mg/kg/day 48 hours after the procedure. High bleeding risk: Enoxaparin 40mg Daily start 24 hours after the procedure. Very high bleeding risk: No post-procedure enoxaparin Resume warfarin the day of procedure; post procedure enoxaparin orders will be discontinued when patient’s INR is within the established therapeutic range on two consecutive days. Other instructions/orders: Physician: Signature: Date: / / Time: Note: Outpatient prescriptions for enoxaparin may be ordered by clinic staff per your authority according to these orders. Fax to 860-425-8791