Diabetes Template - Blue Cross and Blue Shield of North Carolina
advertisement

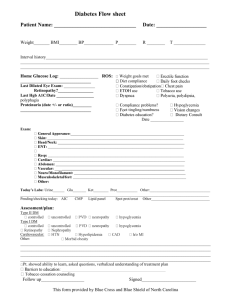
Diabetes Flow sheet Patient Name: _______________________________ Date: ___________________ Weight_______ BMI________ BP_____________ P________ R ________ T ______________ Interval history______________________________________________________________________________ ___________________________________________________________________________________________ ___________________________________________________________________________________________ Home Glucose Log: _________________ ROS: __________________________________ Last Dilated Eye Exam: _______________ Retinopathy?_________________ Last Hgb A1C/Date __________________ polyphagia Proteinuria (date +/- or ratio)_________ __________________________________ Weight goals met Diet compliance e Date ________________ Exam: ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ______________________________________________________________________ _ ____________________________________________________________ Today’s Labs: Urine______ Glu_______ Ket________ Prot___________ Other:________________________________ ____________________________________________________________________________________________________ Pending/checking today: AIC CMP Lipid panel Spot prot/creat Other_______________________________ Assessment/plan: Type II DM Type I DM Cardiovascular: Other: ____________________________________________________________________________________ ____________________________________________________________________________________ ____________________________________________________________________________________ ____________________________________________________________________________________ Pt. showed ability to learn, asked questions, verbalized understanding of treatment plan _____________________ Tobacco cessation counseling Follow up___________________ Signed________________________ This form provided by Blue Cross and Blue Shield of North Carolina



![Detection of proteinuria[1]](http://s3.studylib.net/store/data/007549979_2-02bd2c299a632d6a55125f2f2a73449c-300x300.png)