Parent/Guardian Authorization
advertisement

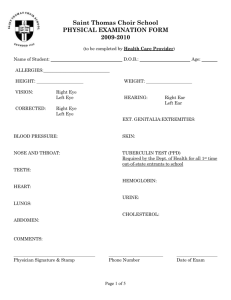
1 of 4 Saint Thomas Choir School PHYSICAL EXAMINATION FORM 2008-2009 (to be completed by Health Care Provider) Name of Student: D.O.B.: HEIGHT: VISION: CORRECTED: Age: WEIGHT: Right Eye Left Eye HEARING: Right Ear Left Ear Right Eye Left Eye EXT. GENITALIA: BLOOD PRESSURE: EXTREMITIES: NOSE AND THROAT: SKIN: TEETH: TUBERCULIN TEST (PPD) Required by the Dept. of Health for all 1st time out of state entrants to school HEART: HEMOGLOBIN: LUNGS: URINE: ABDOMEN: CHOLESTEROL: COMMENTS: Physician Signature & Stamp Phone Number Date of Exam 2 of 4 Name of Student: IMMUNIZATION RECORD The New York City/State Department of Health requires that parents supply evidence of the following immunizations for each child prior to school entrance. Please fill in the spaces with the date each dose was given. In addition, your doctor must sign this immunization record. No child may attend school in New York City without this information. Diphtheria/Tetanus/Pertussis (DPT, DT or Td): 5 (or more) doses required provided 4th dose was given after 4th birthday Date 1st: Date 2nd: Date 3rd: Date 4th: Date 5th: Td: booster within last 10 years Date: H. Influenza Type B. (Hib) Date 1st: Date 2nd: Date 3rd: Oral Poliovirus (OPV or EIPV): birthday Date 1st: Date 2nd: Date 4th: 3 doses required provided third dose was given after 4th Date 3rd: Date 4th: Measles/Mumps/Rubella (MMR): 2 doses required after age 12 months Date 1st: Date: 2nd: Varicella Date: Mantoux PPD (TB) Date: Results: Positive Negative (continued on next page) 3 of 4 Name of Student: Hepatitis B vaccine (Hep B): (3 shots required) recommended at 11-12 years of age for children not previously vaccinated. Date 1st: Date 2nd: Date 3rd: Meningococcal meningitis immunization is recommended for residential students in grades 7 - 12. Please discuss with parent/guardian. I have reviewed the student's immunization record and TB test and find them up-to-date: Health Care Provider’s Name ____________________________________________________ Business Address _____________________________________________________________ Street City State Zip Telephone (____)_____________ Signature of health care provider Date 4 of 4 Saint Tho Saint Thomas Choir School PHYSICIAN’S ORDER FORM 2008-2009 Authorization for the daily administration of medicines by St. Thomas Choir School nurses. St. Thomas Choir School requires a physician's written order and parent or guardian's authorization for the school nurses to administer prescription and over-the-counter medications, including vitamins. Name of Student: DOB: Name, dosage & frequency of medication: ________________________________________________________________________________ Condition for which the drug is being administered: _______________________________ Relevant side effects to be observed (if any): If side effects develop, plan of management: Is this a controlled substance? ______ If yes, DEA number: _____________ Dates for drug to be administered: from _________________ to _________________ mo/day/year mo/day/year Signature of Health Care Provider Date Business Address Phone Parent/Guardian Authorization I hereby request that the above medication, ordered by the above named health care provider for my child, be administered by the school nurses. I understand that I must supply the school with the prescribed medication in the original container in which it was dispensed and it is properly labeled by a physician or pharmacist. I will provide no more than a 45 school day supply of said medication. I understand that this medication will be destroyed if it is not taken home within one week following the termination of the order or beyond the close of school. Signature of Parent/Guardian Address Relationship to child Phone 5 of 4 Saint Thomas Choir School PHYSICIAN’S ORDER FORM #2 2008-2009 Authorization for occasional over-the-counter medication administration by St. Thomas Choir school nurses. St. Thomas Choir School requires the child’s physician and parent/ guardian’s consent for the school nurses to periodically administer over-the-counter medications to students for minor ailments such as toothache, colds, headache, stomachaches, muscle aches and pains, rashes, etc. This will include medications that you may administer in your own home such as Tylenol, Ibuprofen, ambersol, calamine lotion, cough syrup, bacitracin ointment, tums, hydrocortisone cream 1%, benadryl, etc. Medication doses will be calculated by the nurse to be weight and age appropriate for each child. Name of Student:_______________________________________ DOB:__________________________ I hereby authorize the nurses of St. Thomas Choir School to administer over-the-counter medications to the above mentioned student at their discretion for minor ailments. Doses shall be calculated according to weight and age of this child at the time of dispensing. If the child is currently prescribed a medication which may interact with regular over-the-counter medications, or if the child has a pre-existing condition that prohibits his use of certain over-the-counter medications, please list them here. __________________________________________________________________________________________________ __________________________________________________________________________________________________ __________________________________________________________________________________________________ Name of Physician:_____________________________________ Signature of Physician___________________________________ Name of Parent_________________________________________ Signature of Parent______________________________________