Hay fever Treatment Request Form
advertisement

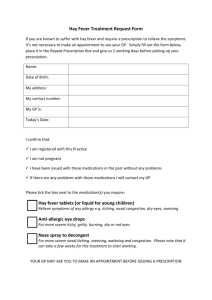
Hay fever Treatment Request Form If you are known to suffer with hay fever and require a prescription to relieve the symptoms it’s not necessary to make an appointment to see your GP. Simply fill out the form below, place it in the Repeat Prescription Box and give us 2 working days before picking up your prescription from Reception. Patient’s Name: DOB: Address: Tel. No.: My GP is: Today’s date: I confirm that: I am a registered with this practice I am not pregnant I have been issued with these medications in the past without any problems If there are any problems with these medications I will contact my GP Please double click and check the box next to the medication(s) you require: Hay fever tablets (or liquid for young children) Relieve symptoms of any allergy e.g. itching, nasal congestion, dry eyes, sneezing Anti-allergic eye drops For more severe itchy, gritty, burning, dry or red eyes Nose spray to decongest For more severe nasal itching, sneezing, watering and congestion. Please note that it can take a few weeks for this treatment to start working. Your GP may want to discuss your request with you, so please provide a telephone number.