Open Access version via Utrecht University Repository
advertisement

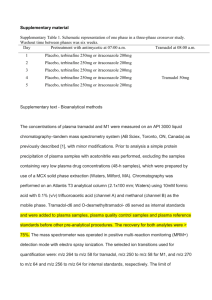
Pharmacokinetic study of oral Once Daily Tramadol compared to Immediate Release Dosage Form of Tramadol in dogs. Abstract Background: Tramadol is used as an analgesic in dogs. A regimen of 3-4 times daily, 2-5 mg/kg is used, but hard to follow. Therefore the aim of this study is to determine whether the immediate release (IR) regimen can be replaced by once daily (OD) formulation, by comparison of the AUC0-24h. Methods: a crossover design with 6 female Beagle dogs. Four times daily 50 mg (2.96 – 3.76 mg/kg) was compared to once daily 200 mg (11.83 – 15.04 mg/kg). Blood samples were analyzed for tramadol, M1, M2 and M5 with a validated LC-MS method. Results: No M1 was found in the dogs and tramadol concentrations are low for IR en OD (59 μg/L and 172 μg/L respectively). There was no statistical significant difference in the AUC0-24h between the two dosage forms. Especially M2 was found. Discussion: Based on these results we could conclude that the IR regimen is replaceable by the OD formulation, however these results have marginal comments, because of possible other active metabolites, small research group and large inter-individual pharmacokinetic differences. Introduction Tramadol hydrochloride, 1RS,2RS-2[(dimethylamino)-methyl]-1-(3-methoxyphenyl)cyclohexanol, is a centrally acting, synthetic analgesic. Tramadol is used in chronic pain and moderate to severe pain, for example postoperative- and benign pain. Non-steroidal anti-inflammatory drugs (NSAIDs) are the only registered drugs in the Netherlands for post-operative analgesia in dogs.3 However, in some cases there is a contra-indication for NSAIDs. For example in patients with renal or gastro-intestinal problems, or when a non-opioid analgesic is not sufficient at its maximum dose. In these cases tramadol is often the drug of choice. As tramadol is not registered as veterinary drug, immediate release (IR) capsules, registered for humans are used.15 The dosage used in dogs is 3 to 4 times daily 2 – 5 mg/kg.19,23 Yazbek et al have shown that tramadol offers equal or significantly better analgesia in post-operative pain in dogs, compared to NSAIDs. 27 The analgesic mechanism of tramadol is mainly achieved by acting on the mu-receptor, but also by inhibiting reuptake of serotonin and norepinephrine.13 The different isomers of tramadol HCl have a different contribution to the analgesic effect. (+)-Tramadols affinity for µ-receptor binding is 20 times larger than that of (-)-tramadol. Furthermore, (+)-transtramadol interacts with adrenergic and serotonergic receptors, while (-)-tramadol only interacts with adrenergic receptors. 22,28 In the liver, tramadol is metabolized by cytochrome P450 (CYP) enzymes8 into phase I metabolites, like Odesmethyltramadol (M1), N-desmethyl-tramadol (M2) and N,O-didesmethyltramadol (M5), all of which are also racemic mixtures13 . Although in different species investigated, the biotransformation of tramadol is qualitatively the same. The metabolites are formed in different quantities2,11,15,16. In canines mainly M2 and M5 are formed9,10,12,15, while in humans high levels of M1 are found1,24. This is of interest, because M1 is the only metabolite that has a more potent μ-receptor binding than tramadol2,9,11,12,13,22. In animal models, (+)-M1 has 6 times the potency of tramadol in providing analgesia and 200 times more potent μ-receptor binding22. (+)-M1 also interacts with adrenergic and serotonergic receptors. By inhibiting the reuptake of serotonin and noradrenalin, tramadol and M1 potentiate their own opioid effect 22. M2 and M5 are qualified as inactive metabolites. (+)M5 has a higher affinity for the μ-receptor than (+)-tramadol, but does not penetrate the blood brain barrier13,29. The µreceptor binding of tramadol is approximately 10-fold less than that of codeine and 6000-fold less than that of morphine. M1 affinity is about 300 times stronger than tramadol, but still has a lower affinity for the receptor than morphine. This accounts for the fact that few adverse events are found in the therapeutic use of tramadol, compared to the effects such as nausea and vomiting caused by other opioids 13. Also constipation, a very common side effect of opioids, is minor with tramadol. Intravenous tramadol had a smaller inhibitory effect on gastric emptying compared to codeine en morphine5,13. These characteristics, of being well-tolerated, less dependence and minor adverse effects, make tramadol a very useful and save-to-use analgesic, which has proven its effect on moderate to severe pain in humans13. The dose given in dogs is higher than in humans. Dogs receive 2-5 mg/kg 3-4 times daily, while in humans 50-100 mg, 3-4 times daily is used. With an average weight of 70 kilograms, that is 0.7-1.4 mg/kg, 3-4 times daily7,19. The elimination half-life of tramadol after oral dosing is 5.5 hours in man 13,15, opposed to 1.71 ± 0.12 h in dogs7,15,19. The systemic clearance is about 5 times faster in dogs compared to humans12,15,29. This explains the higher dose needed in dogs to establish the same analgesic effect. Although a 4-times daily schedule appears to be sufficiently analgesic 20,27, this regimen is hard to follow for a lot of dog owners. A review study in humans found a mean compliance of 71 ± 17%, which declined as the number of doses per day increased4. In the once-daily routine, a compliance of 79 ± 14% was found, compared to 51 ± 20% with a four times daily routine, which is a significant difference4. A study into owner compliance found that, although 70-80% of the owners administered the right number of doses each day, only 20-34% gave doses at the correct time18. Therefore, sufficient pain relief cannot be guaranteed. Because of the need for continuous pain relief during a day and for user friendliness, there are also controlled release tablets registered for human use. These need to be administered only once daily (OD), thereby reducing adverse effects, such as nausea, dizziness, drowsiness and fatigue, due to abrupt peaks in plasma concentrations. The risk of break-through pain is also diminished because of the uniformity of tramadol plasma concentrations6. A study with patients suffering from chronic non cancer pain, reported a significant reduction in pain intensity with controlled release OD tramadol compared to IR tramadol 2. Obviously, the use of OD tramadol has several advantages over IR tramadol, like a more compatible dosage regime for the owners4,18 and a more uniform plasma concentration profile6 . The aim of this study is to determine if the human OD formulation can be used in dogs. In other words, can it achieve a plasma concentration of tramadol (and its (active) metabolites), similar to that obtained by the currently used schedule of IR 4 times daily. We assume that the total 24 hours Area Under Curve (AUC) of tramadol and its metabolites M1, M2 and M5 of the OD dosage form is a representative parameter to establish whether this goal is achieved. Materials & methods Animals Four adult female beagle dogs and two adult female Beagle X Bedlington terrier cross breed dogs, weighing between 13.3 and 16.9 kilograms are used in this study. The mean age of these dogs is 6 years (4-7 years). The study protocol was approved by the Animal Ethical Committee of the Utrecht University. Experimental protocol The setup of this study is a cross-over design. The order of the two treatments, IR-OD or OD-IR, was randomly assigned. Food was given once a day in the morning. Water was available ad libitum. For comparable results between the two dosage forms the concentrations of tramadol needs to be measured at steady state. On the first day, the three dogs of the IR-OD group received one tramadol IR capsule 50 mg (2.96 – 3.47 mg/kg ) every 6 hours, 5 times total. The half life of tramadol in dogs is 1.71 hours, administration of 50 mg IR tablets 4 times daily during 24 hours, to approach a steady state. After the fifth capsule, blood samples are collected at 15/30/45/60/90 and 120 minutes and 4 and 6 hours. At day three and four, tramadol Once Daily 200 mg tablet (11.83 – 13.89 mg/kg per day) is administered. After the second dose, blood samples are collected at 30/60/90 minutes and 3/6/9/15/24 hours. The three dogs of the OD-IR group received tramadol OD 200 mg tablet, once daily (12.12-15.04 mg/kg/day) during 48 hours. After the second dose, blood samples are collected at 30/60/90 minutes and 3/6/9/15/24 hours. Following a 48 hours break, one tramadol IR capsule 50 mg (3.03-3.76 mg/kg) every 6 hours 5 times total, is administered. After the fifth dose, blood is collected at 15/30/45/60/90 and 120 minutes and 4 and 6 hours. Blood sampling Samples were collected by puncture of the jugular vein, using a 22G needle. Blood, 2.5 mL per sample, was collected in plastic serum tubes. The blood was stored on ice until centrifugation at 2000 rpm for 10 minutes and serum was stored in the freezer (minus 15 - 25 degrees Celsius). Chromatography Samples were analyzed by a validated LC-MS method for T (mass to charge ratio (m/z) of 306.2±0.5) and its metabolites M1 (m/z 250.2±0.5), M2 (m/z 250.2±0.5) and M5 (m/z 236.2±0.5). The LC-MS system consisted of a Finnigan Surveyor MS Pump (Thermo Scientific), Surveyor autosampler (Thermo Finnigan) and TSQ Quantum Thermo Finnigan, detected with ‘single ion mass’ (SIM) detection. A run takes 3.6 minutes, injection volume is 5 µl and the system has a flow rate of 300 µL/min. The column used was a HyPURITY AQUASTAR Dim (mm) 50 mm x 2,1 mm inner diameter, particle size 5 µL (Thermo Scientific). The mobile phase consisted of 5% TFA buffer for LC-MS (ammoniumacetate p.a. 5 g/L; acetic acid 100% 35 ml/L; trifluoracetic acid anhydride 2 ml/L, pH 3.5), acetonitrile (Biosolve) and aqua for HPLC (Biosolve). The concentration of acetonitrile (MeCN) and aqua for HPLC differs during the run, the gradient is shown in figure 2. Figure 1: mobile phase gradient Sample preparation To 100 µl serum 750 µl precipitating reagent is added and a sediment was formed. The precipitating reagent consists of 0.04 mg/L cyanoimipramine (internal standard for basic compound), 0.4 mg/L butobarbital (internal standard for acid compounds), 160 ml/L methanol and 840 ml/L acetonitrile. The samples were mixed for 1 minute with a multitube vortexer (Lab-tek Corportion Ltd). Subsequently they were frozen by placing them into the freezer for 30 minutes, followed by shaking them again with the vortex for 1 minute. Finally the samples were centrifuged at 11000 rpm for 5 minutes and collected in the auto sampler of the LC-MS system. Method validation The method validation is implemented as described in appendix 1. The validation results demonstrate that the response for T, M1, M2 and M5 was linear from 5 till 3000 µg/L, the regression coefficients (R2) were 0.99950, 0.99868, 0.99907 and 0.99837 respectively. The accuracy and precision are within the maximum tolerated bias and coefficient of variation (CV) (20% for LLOQ and 15% for the other concentrations), as shown in appendix 2. Also the freeze-thaw stability suffice, this is also summarized in appendix 2. The limit of quantification (LLOQ) for as well tramadol as M1, M2 and M5 is 5 μg/L. The validation process is accomplished in human serum while the samples are in dogs serum. So a cross-validation to dogs’ serum is required for validated results of bloodsamples from dogs. Also the results of the cross-validation met the requirements (an overall bias < 15%), see appendix 3. Pharmacokinetic analysis The pharmacokinetic parameters were analyzed with Excel (Microsoft Office 2007). The area under the curve (AUC0-6h and AUC0-24h) was calculated using the trapezoidal rule. For the immediate release formulation the AUC was multiplied by 4 to extrapolate the AUC to 24 hours, before evaluation and statistical analysis took place. The highest and lowest observed plasma concentration (Cmax and Cmin), time required to reach the maximum plasma concentration (Tmax) and elimination half-life (T1/2) were estimated from the graphs obtained in Excel. The estimated T1/2 is not corrected for absorbtion, so this is not the real T 1/2. Normally the T1/2 of two different dosage forms will be the same, but without the correction for absorption we will expect a higher T1/2 for the OD formulation than the IR formulation. Statistical analysis SPSS was used to perform the Wilcoxon Signed Rank Test and to draw the boxplot. Values of p < 0.05 were considered to be statistically significant. Results After oral administration of tramadol immediate release and the once daily formulation, tramadol was largely metabolized in M2 and M5. The metabolite M1 is also formed, but in very small quantities in comparison to M2 and M5. In the present study, M1 stayed below the lowest limit of quantification (< 5 µg/ml) in all dogs, data not shown. The plasma concentration time curves of tramadol immediate release and once daily are shown in figure 3 and 4. The shape of the graphs differs between the six dogs, especially in the OD formulation. The concentrations of IR tramadol found in dog 5 are much higher than in other dogs, maximum concentration of 220 μg/L in dog 5 versus ± 40 μg/L in the others, see also table 1. After administering the OD formulation, tramadolconcentration were not found in dog 1, while the concentration of tramadol in dog 4 rises high above the others (380 μg/L). As expected, the time to reach maximum concentration (Tmax) of the OD formulation is much longer than of the IR formulation, 9 hours versus 1.5h respectively. Figure 2: concentration time curve tramadol IR (n=6) Figure 3: concentration time curve tramadol OD(n=5) *For dog 3 and 6 concentrations of tramadol at 360 minutes are below LLOQ *For dog 6 only at six, nine and 15 hours the concentration tramadol is above LLOQ *For dog 3 the concentration of tramadol at 24 hours is below LLOQ *For dog 1 the concentration of tramadol did not rise above the LLOQ The plasma profiles of M2 are presented in figure 5 for immediate release and figure 6 for once daily administrations. Figure 5 shows concentration time curves for the 6 dogs with a comparable shape. The shape of the concentration time curves in figure 6 differs remarkably, while dog 1 presents a maximum plasma concentration of 80 μg/L, dog 4 reaches plasma concentrations of 600 μg/L. Figure 4: concentration time curve M2 IR (n=6) Figure 5: concentration time curve M2 OD (n=6) *The concentration of M2 in dog 1 at 24 hours is below LLOQ The plasma concentration curves for M5 are shown in figure 7 for IR and figure 8 for OD. As with the other IRcurves, the shapes between the different curves are comparable, while those in the OD-curves are not. The IR concentration time curve of M5 shows the highest concentrations in dog 5 and the lowest in dog 1. Also in the OD concentration time curve the lowest concentration of M5 is found in dog 1. Figure 6: concentration time curve M5 IR (n=6) Figure 7: concentration time curve M5 OD (n=6) *The concentration of M5 in dog 1 at 24 hours is below LLOQ Figure 9 and 10 show the average concentration time curves of T, M2 and M5 in IR- and OD-formulations. Tramadol’s plasma concentration in both formulations is much lower than that of its metabolite M2. While the concentration of M5 is almost equal to tramadol in the IR tablets, in the OD formulations the concentration of tramadol is higher than that of M5. The time to reach maximum plasma concentration of tramadol, M2 en M5 are almost equal, 1.5-2 hours for IR formulation and 9 hours for OD, as specified in table 1. Other specific pharmacokinetic parameters are also presented in table 1. Figure 8: averages of T, M2 and M5 of IR formulation Figure 10: averages of T, M2 and M5 of OD formulation Table 1: pharmacokinetic variables of tramadol, M2 and M5 Tramadol M2 M5 IR OD (n=5) p-value IR OD p-value IR OD p-value Cmax (µg/L) 59 172 0.225 265 267 0.686 51 57 0.917 Cmin (µg/L) 9 24 0.593 130 46 0.028* 36 28 0.08 Tmax (min) 90 540 0.042* 120 540 0.028* 90 540 0.027* T1/2 (min) 125 270 0.104 250 660 0.028* 345 885 0.028* AUC0-24h (min*μg/L) 41210 103665 0.5 377212.5 247440 0.249 63090 63735 0.753 *: statistic significant difference As shown in the table above, the AUC’s of tramadol, M2 and M5 do not differ significantly between IR en OD. However the AUC for tramadol OD is 2.5 times larger than for tramadol IR, while the AUC for OD M2 is 1.5 times smaller than for IR. The AUC for M5 is approximately the same for both formulations. The maximum serum concentration of tramadol (Cmax) in the once-daily formulation is higher than in the IRformulation, 172 µg/L versus 59 μg/L respectively, though it is not statistic significant (p= 0.225). On the other hand the Cmax~for M2 and M5 reach approximately the same level in both formulations. The not for absorption corrected elimination half time (T1/2) differs, as would be expected, between the two dosage forms and between tramadol and its metabolites. The T1/2 for tramadol does not differ significantly for the different regimens, but they do for M2 and M5. The Tmax of tramadol, M2 and M5 differs statistically significant between de IR and OD formulation, p=0.042 , p=0.028 and p=0.027 respectively. Figure 11 shows a boxplot of the AUC of tramadol for both the IR and OD formulations. This figure shows the difference in variance in the 2 groups. Based on that, the decision was made to use a non-parametric test in this study, because there is no normal distribution of the differences between the AUC of IR and OD. Figure 11: boxplot of the AUC of tramadol in IR and OD formulations. Discussion Our study aimed to find out whether the human OD formulation of tramadol is bioequivalent to the four times daily immediate release regime in dogs. This bioequivalence has to be demonstrated by no significant difference in the 24 hours AUC of tramadol between the IR and OD formulation. The 24 hours AUC of IR tramadol and the OD formulation analyzed in this study show no statistical differences between both dosage forms. Also the Cmax for tramadol, M2 and M5 does not differ significantly between IR and OD. The T1/2 for tramadol does not differ significantly, but for M2 and M5 it does. Although not significantly different, the T1/2 of tramadol for the IR formulation is about twice that of the OD formulation. Further on, we will discuss this result. Based on that, we could state that 50 mg IR capsule tramadol 4 times daily is replaceable by 200 mg OD tablet of tramadol. However, these results should be interpreted with care. Firstly because M1, assumingly the only active metabolite in humans and 200 times more potent than tramadol, is found in the present study in unquantifiable amounts (<5 μg/L). Higher levels of M2 (130 μg/L) and M5 (36 μg/L) were found, which agrees with studies in dogs by Kukanich and Giorgi 9,10,12,15. Also horses formed M1 in unquantifiable amounts en higher levels of M2 and M511. Despite of this lack of M1, studies by Pogge and Yazbek have shown evidence of similar or improved analgesia of tramadol compared to NSAIDs 20,27. Also, observations by experts worldwide have shown tramadol to be clinically relevant in analgesia. One of the possible explanations of this analgesic effect is that other metabolites are (more) active, like M2, M5 or other non studied metabolites. Another possibility is that lower concentrations of T and M1 are therapeutic in dogs. The low amount of M1 can be explained by the so-called flip-flop effect9,10,12,15, in which the elimination of M1 or metabolism of M1 into other metabolites, is faster than the formation of this metabolite (see figure 1). The shorter half-life of tramadol in dogs compared to humans proves that elimination and metabolism of tramadol is faster in these species. Possibly in dogs and other animals the assumption of M1 and tramadol as only active compounds is rejectable. The concentrations of M1 below LLOQ, low levels of tramadol and higher levels of M2 and M5 combined with the proven effectiveness of tramadol in dogs in daily practice suggests that also M2 and M5 are possible active metabolites. M2 penetrates through the blood-brain-barrier (BBB) where it can bind to μ-receptors. Although M5 doesn’t pass the BBB, because it high polarity (Grond), it might be effective, because its affinity for the peripherical μ-receptor17. Mousa et al.17 demonstrated that μ-receptors are formed peripherally at places of chronic pain. Otherwise these metabolites could be effective by serotonergic and/or adrenergic effects. The efficacy of the concentration of tramadol could be questioned. The Cmax of tramadol of 59 μg/L is far below the therapeutic concentration of tramadol in humans (298 μg/L). Only once a concentration of tramadol of over 298 μg/L is reached in a dog during this study. However there are no therapeutic concentrations of tramadol or any metabolites defined for dogs. Based on the proven effectiveness of tramadol IR, we can assume that the concentrations of tramadol, M2 and M5 measured from the IR tablets in this study are effective. Given the fact that not only the AUC but also the Cmax of tramadol, M2 and M5 in the OD form are increased compared to the IR formulation, the OD formulations reaches concentrations above the C max of the IR formulation, and should be effective. Secondly, although the 24 hours AUC of tramadol in both dosage forms doesn’t differ statistically significant, the AUC of the OD regime is even 2.5 times larger than the AUC of de IR regime. The group of dogs used in this study is probably too small, so this makes the probability of obtaining statistically significant differences also quite small, even more so because the inter-individual differences are quite large. By using the Wilcoxon Signed Rank test on every parameter, there is always a 5% change of measuring in the outskirts of the distribution in every test. These pharmacokinetic differences between dogs could be explained in different ways. Primary, feeding could have an influence on the absorption of tramadol. The dogs were fed once a day in the morning. However, the way the dogs were housed influences the time of food intake. Dogs, housed individual, ate the food during the whole day, while dogs sharing a kennel consume their food at once. Giorgi et al. found that food intake did not have a significant effect on biological availability in horses and Raber found the same for people, however in dogs no such reports were found 11,21. Also the metabolism of tramadol and its metabolites seems to influence the pharmacokinetic profile. For example, in one dog low amounts of tramadol were found in IR formulation and in the OD formulation, tramadol even stayed undetected in this dog, also the concentrations of M2 and M5 were rather low. Since CYP2D enzymes are known to be polymorphic, this dog may be an extensive/ultra-rapid metabolizer. In the other dogs metabolism rates could play a role in the differences between pharmacokinetic profiles as well. Beagle dogs are thought to have lower amounts of CYP2D-enzymes, which metabolize tramadol to M1. The metabolism rate of CYP2B and CYP3A in these dogs is higher than that of CYP2D, so more M2 is formed and more M1 and M2 is transformed to M514. Though Kukanich et al.15 also used beagle dogs for their study in tramadol, the choice of beagle dogs for this research could be questioned. Some researchers have found gender differences in the expression of CYP450 enzymes in humans. Besides, females usually have lower body weight and a higher fat percentage, which influences volume of distribution. So using only female dogs, might show different results compared to when male or mixed gender subjects are used25,26. Finally the dosage interval used in dogs is based on the intervals used in humans. However, elimination half-time for tramadol in dogs is remarkably shorter than in human patients, 1.7 hours versus 5.5-6 hours respectively 13,15. Therefore one could question whether or not dosing tramadol 4 times a day in the dog is sufficient. The mean elimination half-life of tramadol in the IR formulation is about half of the elimination half-life of tramadol in the OD formulation. The T1/2 of M2 and M5 are larger for OD than for IR and they differ statistically significant from each other, as can be expected when using an IR and an OD formulation. The same goes for the Tmax of tramadol and its metabolites. Based on that, one could speculate that the dosage interval can be half of that used with IR formulation. This would mean that the OD 200 mg tablet for humans can be used as twice daily tablets for dogs. This could however create a risk of overdosing. A clear-cut effective regimen of dosing OD tramadol twice daily in the dog is rather hard to demonstrate. It would be very useful to obtain information about a minimum and maximum therapeutic concentration of tramadol in the dog. This could then be used to asses analgesic capacity of the OD tablets, based on exact numbers. We assume that the 2-5 mg/kg, 3-4 times daily creates concentrations which are therapeutic, but the concentrations and parameters that were found differ remarkably between dogs. Conclusion In summary the OD formulation of tramadol is compared to the IR formulation for the first time. The AUC 0-24h, Cmax and T1/2 for T, M2 and M5 do not differ significantly between the two dosage forms, excepting the T1/2 of M2 and M5. Based on these results we state that the 50 mg tramadol capsule (four times daily) is replaceable by 200 mg of OD tramadol. However, we have only used tramadol, M1, M2 and M5 as parameters, while possibly other metabolites are active in the dog. We assumed that not only M1 is an active metabolite but also others could be active. Further research in efficacy of different metabolites has to be done to prove this assumption. Because the therapeutic concentrations of tramadol and its metabolites in dogs are unknown, the minimum and maximum active concentration has to be determined before we could state that administrating OD tablets, once or twice daily, is effective. Besides these two disadvantages of our study, we have only used female Beagle (crossbreed) dogs. The results have shown that the inter-individual differences are quite large. Also the group of dogs used in this study is very small, which influences the pharmacokinetic results and the statistics analysis. To extrapolate these results to other genders and breeds and to create reliable results, further research with a larger research group is recommended. Acknowledgements We thank Ies Akkerdaas, Esther Winter, Inge van Geijlswijk and Frits Flesch for their guidance with this study, the employees of the kennel for their help with bloodsampling, friends for accompanying during stays at the kennel, both day and night, and the employees of University Hospital Pharmacy Groningen, with special regards to Remco Koster, for validating and analyzing the bloodsamples. We also like to thank Hans Vernooij for his support with statistics, Robbert Jan Kok for his support with pharmacokinetic analysis and Willy van den Bogaard. Reference list 1. Ardakani Y.H., Rouini M.R. Pharmacokinetics of Tramadol and its Three Main Metabolites in Health Male an Female Volunteers. Biopharmaceutics & Drug Diposition 2007; 28:527-34 2. Beaulieu A.D., Peloso P., Bensen W., Clark A.J., Watson P.N., Gardner-Nix J.,Thomson G., Piraino P.S., Eisenhoffer J., Harsanyi Z., Darke A.D. A randomized, double-blind, 8-week crossover study of once-daily controlled release tramadol versus immediate-release tramadol taken as needed for chronic non-cancer pain. Clinical Therapeutics 2007;29(1) 3. College ter Beoordeling van Geneesmiddelen-Medicines Evaluation Board. 4. Claxton A.J., Cramer J.C., Pierce C. A systematic review of the associations between dose regimens and medication compliance. Clinical Therapeutics 2001;23(8). 5. Crighton I.M., Martin P.H., Hobbs G.J., Cobby T.F. , Fletcher A.J., Stewart P.D. A comparison of the effect of intravenous tramadol, codeine, and morphine on gastric emptying in human volunteers. Anesth. Analg. 1998; 87 (2):445-9 6. Evangelista M. Tramadol sustained release capsules. Drugs 2006;66(2):231-2. 7. Farmacotherapeutisch kompas 2010, geraadpleegd via www.fk.cvz.nl op 22-02-10 8. Gan S.H., Ismail R. Validation of a high-performance liquid chromatography method for tramadol and Odesmethyltramadol in human plasma using solis-phase extraction. Journal of Chromatography B 2001; 759:325-35 9. Giorgi M., Del Carlo S., Saccomanni., Lebkowska-Wieruszewska B., Turini V., Kowalski C.. Biopharmaceutical profile of tramadol in the dog. Vet. Res.Commun. DOI.101007/s11259-009-9278-4. 10. Giorgi M., Del Carlo S., Saccomanni G., Lebkowska-Wieruszewska B., Kowalski C.J. Pharmacokinetic abd urine profile of tramadol ad it’s major metabolites following oral immediate release capsules administration in dogs. Vet Res Commun. DOI 10.1007/s11259-009-9236-1. 11. Giorgi M., Soldani G., Manera C., Ferrarini P.L.., Sgorbini M., Saccomanni G. Pharmacokinetics of Tramadol and its Metabolites M1, M2 and M5 in Horses Following Intravenous, Immediate Release (Fasted/Fed) and Sustained Release Single Dose Administration. Journal of Equine Veterinary Science 2007;27(11):481-8. 12. Giorgi M., Saccomanni G., Lebkowska-Wieruszewska B., Kowalski C. Pharmacokinetic evaluation of tramadol and it’s major metabolites after single oral sustained tablet administration in the dog: a pilot study. The Veterinary Journal (2008), doi:10.1016/j.tvjl.2007.12.011. 13. Grond S., Sablotzki A.. Clinical pharmacology of tramadol. Clin Pharmacokinet 2004;43(13):879-923. 14. Hojo T., Ohno R., Shimoda M., Kokue E. Enzyme and plasma protein induction by multiple oral administrations of Phenobarbital at a therapeutic dosage regimen in dogs. J Vet Pharmacol Ther. 2002;25:121-127. DOI: 10.1046/j.1365-2885.2002.00385.x. 15. Kukanich B., Papich M.G.. Pharmacokinetics of tramadol and the metabolite O-desmethyltramadol in dogs. J. vet. Pharmacol. Therap. 2004; 27: 239-246. 16. Lintz W., Erlacin S., Frankus E., Uragg H.. Biotransformation of tramadol in man and animal. Arzneimittelforschung. 1981; 31(11):1932-43. 17. Mousa S.A. Zhang Q., Sitte N., Ju R-R., Stein C.. Β-endorphin-containing memory-cells ans µ-opioid receptors undergo transport to peripheral inflamed tissue. Journal of Neuroimmunology. 2001; 115:71-78. 18. Overgaauw P. New developments to improve patient compliance. Tijdschrift voor diergeneeskunde 2007 Jan 15;132(2):59-60. 19. Plumb D.C. Plumb’s veterinary drug handbook. 2005; 5th edition:1113-1114. 20. Pogge S.Q. Tramadol; een alternatief voor postoperatief gebruik van een NSAID voor analgesie bij honden. 2008. 21. Raber M et al Pharmacokinetics properties of tramadol sustained release capsules. 2nd communication: investigation of relative bioavailability and food interaction. Arzneimittelforschung. 1999; jul 49(7):588593. 22. Raffa R.B., Friderichs E., Reimann W., Shank R.P., Codd E.E., Vaught J.L.. Opioid and non-opioid components independently contribute to the mechanism of action of tramadol, an 'atypical'opioid analgesic. The journal of pharmacology and experimental therapeutics 1992;260(1). 23. Robben J.H. Formularium van de Universiteitskliniek voor Gezelschapsdieren, Hond en Kat. Utrecht University. 4e herziene druk, 2001 24. Rouini M.R., Ardakani Y.H., Soltani F., Eboul-Enein H.Y., Foroumadi A. Development and validation of a rapid HPLC method for simultaneous determination of tramadol, and its two main metabolites in human plasma. Journal of Chromatography B 2005; 830:207-11 25. Scandlyn M.J., Stuart E.C., Rosengren R.J. Sex-specific differences in CYP450 isoforms in humans. Expert Opin. Drug Metab. Toxicol. 2008; 4(4):413-424. 26. Tanaka E. Gender-related differences in pharmacokinetics and their clinical significance. Journal of Clinical Pharmacy and Therapeutics. 1999; 24:339–346. 27. Yazbek K.V.B., Fantoni D.T. Evaluation of tramadol, an “atypical” opioid analgesic in the control of immediate postoperative pain in dogs submitted to orthopaedic surgical procedures. Braz. J. vet. Res. Anim. Sci. 2005; 42(4): p 250-258. 28. Wetenschappelijk Instituut Nederlandse Apothekers (WINAp). Informatorium Medicamentorum. 2005. p. 77-8. Analgetica and Antirheumatica. 29. Wu W.N., McKnown L.A., Gauthier A.D., Jones W.J., Raffa R.B. Metabolism of the analgesic drug, tramadol hydrochloride, in rat and dog. Xenobiotica 2001; 31 (7):423-441. Appendix Appendix 1 For method validation two stock solution, stock solution A and B, were prepared by weighing about 1 mg of all components (T, M1, M2 and M5) and solving them in 10 ml blanc human EDTA blood. Resulting in concentrations of all components in the stock solution about 100 mg/L. The calibration curve was prepared from stock solution A. Eight calibration points were used to determine linearity at three different days, these concentrations were 5/25;50;100;200;400;800;1200; 1500 μg/L. For each component a calibration curve was analyzed and the measured regression coefficient (R2) has to be > 0.998 to met the criteria for linearity. Stock solution B was used for the preparation of validation pools. This stock was diluted till ‘high’ (1200 μg/L), ‘medium’ (400 μg/L) and a ‘low’ (75 μg/L) concentrations, which were used for determination of the accuracy and precision. Also a pool for the lower limit of quantification (LLOQ) (5 μg/L) and a dilution pool (over-curve) of 3000 μg/L were prepared from stock B. The over-curve dilution consisted of a single concentration of at least two times the concentration of the highest stock (1200 μg/L). All concentrations were measured in 5-fold in three separate runs on separate days for determination of the accuracy, precision and over-curve dilution. Stabilities of tramadol and its metabolites were assessed at room temperature, in the autosampler and during 3 freeze-thaw cycles. Validation was performed with a maximum tolerated bias and coefficient of variation (CV) of the LLOQ of 20% and 15% for the other validation concentrations. For each validation, concentration bias and CV were calculated per run. Within-run, between-run and overall CVs were calculated using one-way ANOVA. This validation was run in human serum, but the samples are from dogs. This required a cross-validation to dogs serum: the accuracy was repeated but the stock solution used were prepared in blanc blood of dogs. When the overall bias of the within run variation in dogs serum is lower than 15%, there could be assumed that the validation results in human could be extrapolated to dogs. Appendix 2 Table 1: validation results of tramadol, M1, M2 and M5 in human serum Component Tramadol Regression coefficient, linear range (µg/L) 0.99950 (5.00-1500) M1 0.99868 (5.00-1500) M2 0.99907 (5.00-1500) M5 0.99837 (5.00-1500) Concentration (µg/L) LLOQ (5.0) LOW (75.0) MED (400.0) HIGH (1200.0) DIL (3000.0) F/T stab LOW F/T stab HIGH RT stab 152 h LOW AS stab 46 h LOW AS stab 114 h LOW RT stab 152 h HIGH AS stab 46 h HIGH AS stab 114 h HIGH LLOQ (5.0) LOW (75.0) MED (400.0) HIGH (1200.0) DIL (3000.0) F/T stab LOW F/T stab HIGH RT stab 152 h LOW AS stab 46 h LOW AS stab 114 h LOW RT stab 152 h HIGH AS stab 46 h HIGH AS stab 114 h HIGH LLOQ (5.0) LOW (75.0) MED (400.0) HIGH (1200.0) DIL (3000.0) F/T stab LOW F/T stab HIGH RT stab 152 h LOW AS stab 46 h LOW AS stab 114 h LOW RT stab 152 h HIGH AS stab 46 h HIGH AS stab 114 h HIGH LLOQ (5.0) LOW (75.0) MED (400.0) HIGH (1200.0) DIL (3000.0) F/T stab LOW F/T stab HIGH RT stab 152 h LOW AS stab 46 h LOW AS stab 114 h LOW RT stab 152 h HIGH AS stab 46 h HIGH AS stab 114 h HIGH Within run (%) 4.6 4.3 3.0 2.8 1.4 3.9 3.6 3.1 4.0 5.0 1.4 3.2 5.1 6.1 4.9 3.6 3.3 3.4 4.0 4.2 3.6 4.5 3.9 2.2 4.6 4.9 5.8 3.5 3.9 2.4 2.2 3.8 3.5 4.6 2.3 4.6 1.2 3.7 4.6 6.9 5.0 3.6 2.9 2.7 4.1 4.7 3.4 4.4 2.8 7.2 4.1 4.3 Between run (%) 9.4 0.0 0.9 0.4 0.7 1.8 2.8 NA NA NA NA NA NA 8.2 3.4 1.3 0.8 0.0 0.0 1.6 NA NA NA NA NA NA 8.4 3.1 0.4 0.7 1.7 1.0 2.0 NA NA NA NA NA NA 8.9 0.0 0.0 0.3 4.0 0.0 0.0 NA NA NA NA NA NA Overall CV (%) 10.5 4.3 3.1 2.8 1.5 4.3 4.5 NA NA NA NA NA NA 10.2 6.0 3.8 3.4 3.4 4.0 4.5 NA NA NA NA NA NA 10.3 4.6 3.9 2.5 2.7 3.9 4.0 NA NA NA NA NA NA 11.3 5.0 3.6 2.9 4.8 4.1 4.7 NA NA NA NA NA NA Overall bias (%) 1.5 10.3 13.0 7.1 14.0 14.2 10.0 13.8 14.5 18.1 6.8 14.3 12.6 -1.2 10.5 11.0 6.7 13.0 13.2 8.0 14.1 12.3 13.7 5.7 12.4 7.6 -2.8 9.4 11.3 5.1 13.0 12.8 7.0 14.0 15.5 13.6 6.9 11.3 8.9 -3.7 10.6 14.0 9.8 10 16.7 10.0 19.0 15.1 15.9 13.2 12.5 8.2 LLOQ, LOW, MED, HIGH are the validation concentrations used for accuracy and precision; DIL is the dilution pool, which is 10 times diluted before sample preparation; F/T stab LOW, freeze thaw stability of 75 µg/L after 3 cycles; F/T stab HIGH, freezethaw stability of 1200 µg/L after 3 cycles; RT stab xx h: stability in whole blood at room temperature for xx hours; AS stab xx h, stability in the autosampler for xx hours; NA, not applicable. Appendix 3 Table 2: cross-validation results tramadol, M1, M2 and M5 in dogs serum. Component Tramadol M1 M2 M5 Concentration (µg/L) LLOQ (25.0) LOW (75.0) MED (400.0) HIGH (1200.0) DIL (3000.0) LLOQ (25.0) LOW (75.0) MED (400.0) HIGH (1200.0) DIL (3000.0) LLOQ (5.0) LOW (75.0) MED (400.0) HIGH (1200.0) DIL (3000.0) LLOQ (5.0) LOW (75.0) MED (400.0) HIGH (1200.0) DIL (3000.0) Overall (%) 2.2 4.7 3.5 3.2 2.3 4.5 3.9 3.7 3.7 3.2 4.1 4.3 3.9 2.9 1.4 5.4 5.7 2.3 3.2 3.0 CV Overall bias (%) 7.0 12.0 11.3 8.8 8.1 -1.8 12.3 11.8 -4.6 9.6 4.7 7.9 9.0 4.0 13.8 -0.5 9.0 11.7 14.8 13.7