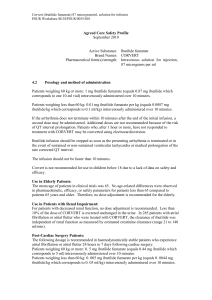
Ventricular tachycardia (or VT) is a tachycardia, or fast heart rhythm
advertisement
 is a tachycardia, or fast heart rhythm")
Ventricular tachycardia (or VT) is a tachycardia, or fast heart rhythm that originates in one of the ventricles of the heart. This is a potentially life-threatening arrhythmia because it may lead to ventricular fibrillation and sudden death. Less commonly, however, some forms of this arrhythmia appear benign, especially in young individuals. Classification of VT Pulseless ventricular tachycardia should be treated as ventricular fibrillation. Ventricular tachycardia with a pulse is classified as stable or unstable, based on the respective absence or presence of symptoms in the patient. Unstable ventricular tachycardia may be defined by one or more of the following adverse signs: systolic blood pressure less than 90 mm Hg pulse rate greater than 150 beats per minute chest pain evidence of heart failure They can also be classified based on its morphology: Monomorphic ventricular tachycardia means that the appearance of all the beats match each other in each lead of a surface electrocardiogram (ECG). Polymorphic ventricular tachycardia, on the other hand, has beat-tobeat variations in morphology. This most commonly appears as a cyclical progressive change in cardiac axis referred to by its French name torsades de pointes ("twisting of the points"). Treatment of haemodynamically unstable VT The steps used in the resuscitation procedure are outlined: provide high flow oxygen establish i.v. access consider sedation or ideally, intubation with general anaesthesia perform cardioversion i.e. synchronised DC shocks o for a monophasic defibrillator, start at 100 J if VT persists, increase to 200 J if VT persists, increase to 360J (if using a biphasic defibrillator, use the equivalent biphasic energy levels) check serum potassium and correct if less than 4 mmol/l: o give up to 60 mmol potassium chloride at maximum rate of 30 mmol per hour if hypokalaemic, assume patient also to be hypomagnesaemic: o give 10 mmol magnesium sulphate over 30 minutes (5 mls of 50% solution) if VT persists, obtain expert help; but consider: o amiodarone 150 mg in 20 mls 5% dextrose over 10 minutes o further cardioversion o other anti-arrhythmics o overdrive pacing o o o Treatment of haemodynamically stable VT. The steps used in the resuscitation procedure are outlined: give high flow oxygen establish i.v. access check serum potassium; if less than 4 mmol/l: o give up to 60 mmol potassium chloride at maximum rate of 30 mmol per hour if hypokalaemic, assume patient also to be hypomagnesaemic: o give 10 mmol magnesium sulphate over 30 minutes (5 mls of 50% solution) give either: o amiodarone 150 mg in 20 mls 5% solution over 10 minutes; OR o lignocaine 50 mg over 2 minutes repeated every 5 minutes up to a maximum of 200mg start a lignocaine infusion at 2 - 4 mg per minute if VT persists, obtain expert help; consider: o cardioversion (i.e. synchronised DC shocks at monophasic energy levels of 100J:200J:360J or biphasic equivalents) o further amiodarone 150 mg in 20 mls 5% dextrose over 10 minutes)