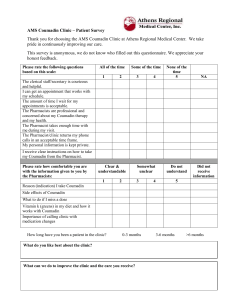
SCOPE Clinic – Patient Screening Form
advertisement

SCOPE Clinic – Patient Screening Form Please fill out: Name: Gender: Date of Birth: Your Height: Your Weight: Daytime Phone #: Home Phone #: Do you have any of the following conditions? Y N Y N Please describe diagnosis where possible: Heart condition Lung condition Stroke/TIA Liver Disease Kidney condition (except stones) Diabetes requiring insulin Malignant Hyperthermia Severe reaction to anesthetics Are you on any blood thinners? Coumadin/Warfarin Plavix Aggrenox Ticlid/Ticlopidine Other: On physical exertion, do you experience the following symptoms? Y Angina/Chest Pain Shortness of Breath N