Request for Reasonable Accommodations
advertisement

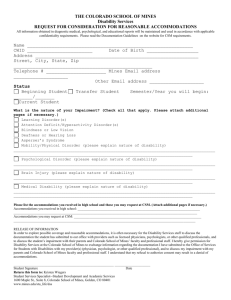
REQUEST FOR REASONABLE ACCOMMODATIONS COLORADO SCHOOL OF MINES STUDENT DISABILITY SERVICES (SDS) Please read the Documentation Guidelines on the website for CSM requirements. All information obtained in diagnostic medical, psychological, and educational reports will be maintained and used in accordance with applicable confidentiality requirements. Name: CWID: Date of Birth: Address: Street, City, State, Zip: Telephone #: Mines Email address: Other Email address: Status: Beginning Student Transfer Student Current Student Semester/Year you will begin: Semester/Year you will begin: Semester/Year you began: Please check all that apply: Attention Deficit/Hyperactivity Disorder(s) Autism Spectrum Syndrome Brain Injury Hearing Impairment Learning Disorder(s) Medical Condition Mobility/Physical Impairment Psychological Disorder Visual Impairment Accommodations you are seeking at CSM: _____________________________________________________________________________________________________________________ RELEASE OF INFORMATION If necessary in order for CSM to provide reasonable and effective accommodations, I hereby give permission for SDS staff to discuss the documentation I have submitted with my physician, psychologist, or other qualified professional, and to discuss my impairment with my parents and CSM faculty and professional staff. I understand that my refusal to authorize consent may result in incomplete information and a denial of accommodations. Student Signature: Return this form to: Student Disability Services W. Lloyd Wright Student Wellness Center, Room 205 Golden, CO 80401 Date: