Diabetes Care Plan
advertisement

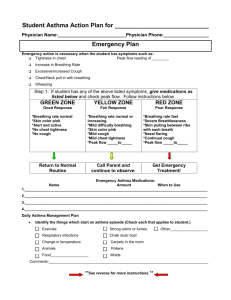
Date Plan was Developed Call School Nurse DIABETES Emergency Care Plan Never send student with suspected low blood sugar anywhere alone!!!!!!!!!!!! Student Name;________________________________________DOB:______________________________ Parent/Guardian:_____________________________ Home Phone:_______________ Work Phone: _____________ Emergency Contact: __________________________ Home Phone:_______________ Work Phone: _____________ Emergency Contact: __________________________ Home Phone: _______________ Work Phone:______________ Student Picture Physician: __________________________________ Phone:_____________________ Preferred Hospital: ___________________________ Current Medication:______________________________________________________________________________________________ Allergies:______________________________________________________________________________________________________ SYMPTOMS AND SIGNS OF LOW BLOOD SUGAR MILD Unable to concentrate Hunger Shakiness Weakness Sweaty Dizziness MODERATE Personality change: Behavior change: Poor coordination Blurry vision Weakness Headache Confusion Drowsy Pale Irritable Anxious *Student’s usual signs/symptoms *Student’s usual signs/symptoms IF YOU SEE THIS SEVERE Loss of consciousness Seizures Stops breathing * Student’s usual signs/symptoms DO THIS Never send student anywhere alone!!!!! MILD TO MODERATE If unable to go to health office, have meds brought to student Sit student in upright position, offer water Instruct to breathe in through nose and out through pursed lips slowly and deeply Check peak flow. Reading:__________ Check time of last does of medication Give medication by inhaler or nebulizer (Specify medication, dose, route) Assist student to inhale medication slowly and fully. Student becomes worse: Will not or cannot Drink or swallow CALL 911 Pull lower lip down and squeeze (glucose gel) between the lower lip and the gum. If student is lying down, turn on side to prevent choking Glucose gel located _______________________________________ Call parent SEVERE SEIZURE BREATHING STOPS TIME Initial Call 911 If possible, adult trained in CPR/Rescue Breathing stays with student until 911 arrives Clear area to prevent injury, place soft material under head Do not hold student down. Do not put anything in mouth. Begin CPR/Rescue Breathing Note time of arrival and departure of ambulance; complete this form, initial, and send a copy of form with the ambulance. The following staff members are trained to deal with an emergency, and initiate the appropriate procedures: 1:________________________________________ 2:____________________________________3:_____________________________ __________________________________________ Registered Nurse’s Signature ___________________________ Date __________________________________________ Parent/Guardian Signature ___________________________ Date