Pancreatic Sonography – Part II - e
advertisement

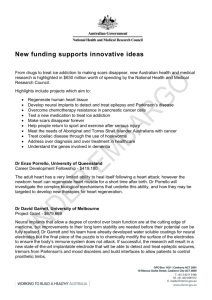
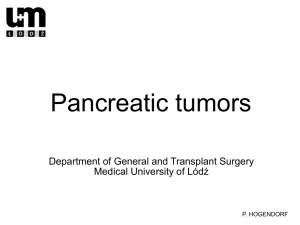
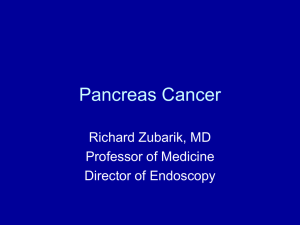
Pancreatic Sonography – Tumors – Updated Author: Philip W. Ralls M.D. Objectives: Upon completion of this CME article, the reader will be able to 1. Discuss the treatment and clinical outcome for pancreatic malignancies. 2. Compare and contrast chronic pancreatitis and pancreatic neoplasms. 3. Describe the application of color Doppler sonography in evaluating pancreatic tumors. Pancreatic Neoplasms Sonography and Computed Tomography (CT) are the primary tools used to detect focal pancreatic disease, especially pancreatic carcinoma. CT is generally superior because it routinely images the entire pancreas. Sonography is also superb when the entire pancreas can be imaged. Occasionally, sonography may delineate pancreatic masses better than contrast enhanced CT. Unfortunately, even with optimal equipment and scanning technique (upright, water filled stomach and duodenum), the entire pancreas can be visualized in only about 25% to 50 % of patients. Sonography is the primary imaging method used in screening patients with jaundice. Ultrasound can usually detect pancreatic carcinoma that obstructs the bile duct and may also identify a pancreatic mass in a patient scanned for abdominal pain. Sonography is occasionally useful in characterizing abnormalities noted on CT, determining for example, whether a lesion is cystic or solid. Pancreatic Ductal Adenocarcinoma Pancreatic ductal adenocarcinoma is by far the most common primary pancreatic neoplasm, comprising approximately 80% of all pancreatic neoplasms and about 90% of malignant epithelial tumors. Pancreatic carcinoma, whose prevalence has tripled during the last forty years, is one of the commonest causes of cancer death in the United States. Pancreatic ductal adenocarcinoma is one of the most lethal malignancies, and the overall five-year survival is poor at 2 % or less. Sonographically, pancreatic carcinoma is typically (about 60 % of the time) a hypoechoic mass that deforms the gland's morphology. Homogeneous masses are slightly more common than heterogeneous masses. In our recent series, about 10% caused no glandular contour abnormality and were visualized only because tumor echogenicity differed from the normal pancreas. Occasionally, pancreatic carcinoma is hyperechoic. Masses with increased echogenicity are common in chronic pancreatitis but rare in carcinoma. Slightly more than 60% of these carcinomas occur in the pancreatic head; about 5 % are diffuse and the remaining 35% are found in the body or tail. Calcification occurs in about 5 % of the masses (figure 1) and is usually focal and scattered, unlike typical chronic pancreatitis calcifications. Small intralesional cysts occur in about 15 % of patients. Pseudocysts, related to obstruction of a pancreatic duct, occur in about 5% to 10 % of patients. Glandular atrophy may occur from obstruction caused by a tumor. The following findings suggest unresectability: tumor larger than 2 cm, extracapsular extension, vascular invasion (venous or arterial), lymphadenopathy, or metastatic disease. As the mortality of the Whipple procedure declines, some surgeons have become more aggressive. Some surgeons now feel that pancreatic head lesions are unresectable only when the superior mesenteric artery is involved or when metastatic disease is present. New trials are needed to see if this more aggressive surgical approach will result in improved survival. Preliminary thick section contrast enhanced CT often reveals evidence of metastasis or other signs of unresectability. If no evidence of unresectability is noted, color Doppler sonography is very useful in assessing vascular invasion and contiguity, which are the usual keys in determining whether a lesion is resectable or not. High-resolution spiral CT and color Doppler imaging can both provide this type of information. Image findings of unresectability are reliable and only rarely can such a tumor be resected if surgery is attempted. Conversely, many tumors believed resectable because of their image appearance on CT or sonography cannot be resected for cure at surgery. Furthermore, the five-year survival of patients undergoing attempted curative resection is only 5% to 8%, although more recent studies have reported five-year survival in the 10% to 20% range. Masses Associated with Chronic Pancreatitis Focal pancreatic enlargement occurs in approximately 30 % of patients with chronic pancreatitis. Carcinoma and chronic pancreatitis related masses can usually be differentiated clinically. In addition, the presence of calcification within a mass makes the diagnosis of pancreatitis almost certain (although a few carcinomas can have calcifications). Hyperechoic masses, even without discrete calcifications, are usually related to chronic pancreatitis. An uncalcified iso or hypoechoic mass is nonspecific. In this instance, biopsy or endoscopic retrograde cholangiopancreatography (ERCP) is indicated to differentiate carcinoma from chronic pancreatitis. Carcinoma and pancreatitis may both cause obstruction of the pancreatic duct or extrahepatic bile duct. Obstruction of both ducts, the "double duct sign", is nonspecific, occurring in both pancreatitis and pancreatic carcinoma. Pseudocysts, while more frequent in pancreatitis, also occur in both conditions. Pancreatic Cystic Disease Cystic pancreatic tumors are relatively uncommon, comprising fewer than 15% of pancreatic cystic lesions and only a few percent of pancreatic tumors. Cystic pancreatic neoplasms include serous cystic neoplasms (microcystic adenomas) and mucinous cystic neoplasms (macrocystic adenomas). Serous cystic neoplasms are almost universally benign, although a malignant variant has been reported. When image findings typical for microcystic adenoma are present, asymptomatic or poor risk patients need not undergo surgery. A serous cystic neoplasm (figure 2) is slightly more common in females and tends to occur in older individuals. Morphologically, serous cystic neoplasms contain many tiny cysts (i.e. microcystic), most of which are smaller than 2 cm. Occasionally, a few larger cysts are present. A distinctive but inconsistent feature is a central stellate fibrotic scar that frequently calcifies (seen in about 50% of tumors). Sonographically, microcystic adenomas are echogenic in regions of the tumor where there are many tiny cysts. Through transmission is frequent. The central stellate scar with calcification may be identified, suggesting the diagnosis. Mucinous cystic neoplasms consist of large cysts (i.e. macrocystic), easily imaged with CT or sonography. Most tumors are located in the tail or body of the pancreas and are much more common in females, approaching a 10 to 1 predominance. Because differentiation between benign and malignant mucinous cystic neoplasms is often impossible even pathologically, all tumors are considered malignant and surgical removal is indicated. Calcifications occur in approximately 20% of these neoplasms (compared to about one half of the serous cystic neoplasms). Sonography can reveal other cystic masses that may be comprised of simple unilocular cysts or septated cysts of variable size. The septations may be few or many, quite thin or relatively thick, and polypoid. Endocrine Tumors of the Pancreas Endocrine tumors are a small but important group of pancreatic neoplasms that generally originate from the pancreatic islet cells. Insulinomas and gastrinomas are the most common endocrine tumors. Other tumors that can originate from the islet cells are glucagonoma, somatostatinoma, vasoactive intestinal peptide tumors (VIPoma), carcinoid tumors, pheochromocytoma, and combined histology tumors. These tumors tend to be small and are malignant, with the exception of the insulinoma. It is difficult to image islet cell tumors because they are usually small when the patient presents with hormonal abnormalities. Insulinomas and gastrinomas are frequently less than 2 cm in diameter. Thin section dynamic incremental contrast enhanced CT or angiography can sometimes reveal these lesions. Intraoperative sonography is useful in localizing occult neoplasms. Published success rates for the detection of insulinomas vary from 25% to 60%. The results for gastrinomas are worse in that approximately only 20% are detected. Sonographically, islet cell tumors are usually well defined and round or oval in shape. They generally appear hypoechoic compared to the normal pancreatic parenchyma. On occasion, the only detectable abnormality may be an alteration of the pancreatic contour. Increased echogenicity from calcification has been reported. Most islet cell tumors are hyperfunctioning. When they are not hyper-functioning, these pancreatic endocrine tumors may grow to a large size before being detected. Metastasis to the Pancreas In autopsy series, the most common pancreatic neoplasm is metastatic carcinoma. Primary tumors that commonly metastasize to the pancreas include breast, lung, colon and stomach cancers, as well as, melanoma. Pancreatic metastases are rarely significant clinically, because they generally occur late in patients who have widespread metastatic disease. Resectability of Periampullar Neoplasms / The Role of Color Doppler The prognosis for pancreatic carcinoma and other pancreatic neoplasms is grim, although periampullar neoplasms (other than pancreatic ductal adenocarcinoma) have a somewhat better prognosis. The only hope for cure remains surgical resection. In the last decade, surgical results have improved and operative morbidity and mortality have decreased. In recent series, resection for cure has been possible in 15% to 20 % of unselected patients and 29% to 34% of patients screened as suitable candidates for curative resection. Sonography is often the first modality used to image patients with pancreatic carcinoma, as these patients usually present with jaundice or abdominal pain. Despite this, little work has been done to assess the usefulness of sonography in evaluating the resectability of pancreatic neoplasms. In most recent discussions of imaging in pancreatic neoplasms, transabdominal sonography has been almost totally ignored. We have developed a technique for assessing the resectability of pancreatic tumors using color Doppler sonography. In a retrospective analysis of 51 patients referred for color Doppler sonographic evaluation of the resectability of a pancreatic neoplasm, 45 had an adequate evaluation with follow-up. Vessels that were touched or occluded by tumor were categorized according to a Pancreatic Color Doppler Score (Table 1). Other factors affecting resectability (metastasis or enlarged lymph nodes) were recorded. Findings were correlated to the surgical and pathologic findings of resectability and unresectability. TABLE 1 - PANCREATIC COLOR DOPPLER SCORE PCDS 0 Tumor did not touch a vessel. PCDS 1 Tumor touched, 1% - 24% around the vessel circumference. PCDS 2 Tumor touched, 25% - 49% around the vessel circumference. PCDS 3 Tumor touched, 50% - 99% around the vessel circumference. PCDS 4 Tumor touched, 100% around the vessel circumference. “Encasement” PCDS 5 Occluded vessel. All 18 patients with circumferential tumor or vascular occlusion (PCDS 4 & 5) could not be resected (figure 3). All of the margins were negative in the 10 patients where the tumor did not touch a vessel (PCDS 0). All 30 patients considered unresectable sonographically were also unresectable for cure based on surgical and pathological information. Six of 15 (40%) that were considered resectable sonographically were unresectable for cure. Color Doppler sonography influenced therapy in 10 of 45 patients (22% overall). Doppler sonography has been found useful in assessing the resectability of other tumors such as cholangiocarcinoma. Our data comprise a feasibility study that suggests color Doppler sonography can greatly enhance the usefulness of sonography in evaluating pancreatic neoplasms. In the important area of determining that a patient cannot be cured by surgical resection, our data showed a positive predictive value of 100%. That is, color Doppler sonography unresectability correlated with all 30 patients who were unresectable for cure. In those cases, no further evaluation would be required. The prediction of unresectability of pancreatic carcinoma with CT scanning is also very reliable; however, our data suggest that color Doppler sonography likewise may be reliable. Identifying patients who are potentially resectable with a high probability for cure is more difficult. One potential problem in using color Doppler sonography to assess resectability of pancreatic tumors is that the examiner must have significant experience in abdominal color Doppler imaging. We have learned, nevertheless, that color Doppler evaluation of patients with pancreatic masses is actually simpler than evaluation of patients with a normal pancreas. Pancreatic neoplasms tend to be non-compressible and are often immobile. Thus, compression with a large footprint curved linear array transducer allows visualization of the mass and its relationship to any vessels. In this study we visualized 643 of 647 possible vessels (99.4 % visualization rate) and achieved complete technical success in 49 of 51 patients (96%). It should also be remembered that the great majority of pancreatic neoplasms occur in the head and body of the pancreas, which are the easiest regions to visualize sonographically. Can color Doppler sonography decrease the need for CT in assessing resectability of pancreatic neoplasms? The role of color Doppler sonography in the evaluation of pancreatic tumors awaits the results of prospective trials. Our data, however, suggest that color Doppler sonography is promising. It was reliable in detecting unresectable lesions in our series, detecting all 30 patients who were unresectable for cure. A “touch/no touch” color Doppler analysis that compared color Doppler findings to tumor free margins showed that when tumor did not touch vessels, the margins were negative (10 of 10 patients). Color Doppler sonography, a comfortable, non-invasive, and relatively inexpensive examination, may be an effective screening tool for evaluating resectability. If color Doppler sonography can correctly predict unresectability, then 80% of pancreatic carcinoma patients would require no further expensive or invasive imaging evaluation, and palliative management could proceed. Thus, only 20% of patients would require further evaluation (such as CT, ERCP, laparoscopy, etc.). Sonography has been almost totally ignored in the most recent discussions regarding imaging in pancreatic and periampullar neoplasms. It seems clear from our data that color Doppler sonography can be very useful in evaluating the resectability of pancreatic neoplasms. Any future evaluation of imaging and management of pancreatic tumors should include color Doppler sonography. Figures 1 Pancreatic Carcinoma with calcification. 2 Microcystic Adenoma (Serous Cystic Neoplasm) 3 Pancreatic Carcinoma encases the superior mesenteric artery – PCDS 4. References or Suggested Reading: 1. Sofuni A, Iijima H, Moriyasu F, et al. Differential diagnosis of pancreatic tumors using ultrasound contrast imaging. J Gastroenterol. 2005;40:518-525. 2. Scialpi M, Midiri M, Bartilotta TV, et al. Pancreatic carcinoma versus focal pancreatitis: contrast-enhanced power Doppler ultrasonography findings. Abdom Imaging. 2005;30:222-227. 3. Rickes S, Malfertheiner P. Echo-enhanced sonography – an increasingly used procedure for the differentiation of pancreatic tumors. Dig Dis. 2004;22:32-38. 4. Alvarez C, Livingston EH, Ashley SW, et al.. Cost-benefit analysis of the work-up for pancreatic cancer. Am J Surg 1993;165:53-60. 5. Angeli E, Venturini M, Vanzulli A, et al. Color Doppler imaging in the assessment of vascular involvement of pancreatic carcinoma. AJR 1997;168:193-197. 6. Cameron JL, Pitt HA, Yeo CJ, et al. One hundred and forty-five consecutive pancreaticoduodenectomies without mortality. Ann Surg 1993;217:430-438. 7. Freeny PC, Traverso LW, Ryan JA. Diagnosis and staging of pancreatic adenocarcinoma with dynamic computed tomography. Am J Surg 1993;165:600-606. 8. Fuhrman GM, Charnsangavej C, Abbruzzese JL, et al. Thin-section contrastenhanced computed tomography accurately predicts the resectability of malignant pancreatic neoplasms. Am J Surg 1994;167:104-113. 9. Geer RJ, Brennan MF. Prognostic indicators for survival after resection of pancreatic adenocarcinoma. Am J Surg 1993;165:68-73. 10. Gudjonsson B. Carcinoma of the pancreas: critical analysis of costs, results of resections, and the need for standardized reporting. J of Am Col Surgeons 1995;181:483-503. 11. Hann LE, Fong Y, Shriver CD, et al. Malignant hepatic hilar tumors: Can ultrasonography be used as an alternative to angiography with CT arterial portography for determination of resectability? J Ultrasound Med 1996;15:37-45. 12. Hough DM, Stephens DH, Johnson CD, Binkovitz LA. Pancreatic lesions in von Hippel-Landau disease: Prevalence, clinical significance, and CT findings. AJR 1994;162:1091-1094. 13. Ikeda M, Sato T, Morozumi A, Fujino MA, et al. Morphologic changes in the pancreas detected by screening ultrasonography in a mass survey, with special reference to main duct dilatation, cyst formation, and calcification. Pancreas 1994;9:508-512. 14. Klinkenbijil, JHG, Jeekel J, Schmitz PIM, et al. Carcinoma of the pancreas and periampullary region: palliation versus cure. Br J Surg 1993;80;1575-1578. 15. Looser C, Stain SC;, Baer HU, Triller J, Blumgart LH. Staging of hilar cholangiocarcinoma by ultrasound and duplex sonography: a comparison with angiography and operative findings. Br J Radiol 1992;65:871. 16. Mathieu D, Guigui B, Valette PJ, et al. Pancreatic cystic neoplasms. Radiol Cl North Am 1998;27:163-176. 17. Megibow AJ, Zhou XH, Rotterdam H, et al. Pancreatic adenocarcinoma: CT versus MR imaging in the evaluation of resectability - Report of the radiology diagnostic oncology group. Radiology 1995;195:327-332. 18. Nghiem HV, Freeny PC. Radiologic staging of pancreatic adenocarcinoma. Radiol Clin North Am 1994;32:71-79. 19. Nitecki SS, Sarr MG, Colby TV, vanHeerden JA. Long-term survival after resection for ductal adenocarcinoma of the pancreas. Is it really improving? Ann Surg 1995;221:59-66. 20. Ralls PW, Wren SM, Radin DR, et al. Color Doppler sonography in evaluating the resectability of periampullar pancreatic tumors. J Ultrasound Med 1997;16:131-140. 21. Tomiyama T, Ueno N, Tano S, et al, Assessment of arterial invasion in pancreatic cancer using color Doppler ultrasonography. Am J Gastroenterol 1996;91:1410-6. 22. Trede M, Schwall G, Saeger HD. Survival after pancreatoduodenectomy. Ann Surg 1990;211:447-458. 23. Vellet AD, Romano W, Bach DB, et al. Adenocarcinoma of the pancreatic ducts: Comparative evaluation with CT and MR imaging at 1.5T. Radiol 1992;183:87-95. 24. Wade TP, El-Ghazzawy AG, Virgo KS, Johnson FE. The Whipple resection for cancer in U.S. department of veterans affairs hospitals. Ann Surg 1995;221:241-248. 25. Wade TP, Radford DM, Virgo KS, Johnson FE. Complications and outcomes in the treatment of pancreatic adenocarcinoma in the United States veteran. J Am Coll Surg 1994;179:38-48. 26. Warshaw AL and Fernandez-del Castillo C. Pancreatic carcinoma. N Engl J Med 1992;326:455-465. 27. Warshaw AL, Gu Z, Wittenberg J, Waltman AC. Preoperative staging and assessment of resectability of pancreatic cancer. Arch Surg 1990;125:230-233. 28. Watanapa P and Williamson RCN. Surgical palliation for pancreatic cancer: developments during the past two decades. Br J Surg 1992;79:8-20. 29. Wren SM, Ralls PW, Stain SC, et al. Assessment of resectability of pancreatic head and periampullary tumors by color Doppler Doppler sonography. Arch Surg 1996;131:812-818. About the Author Dr. Philip W. Ralls is a Professor of Radiology at Keck School of Medicine, University of Southern California. He is an active Radiologist and is a Fellow of the American College of Radiology and numerous other professional organizations. Dr. Ralls has presented numerous lectures on ultrasound topics at many different conferences around the country and is actively involved in research. In addition, he has authored several publications in peer-review medical journals. Examination: 1. When evaluating the pancreas for the presence of tumors, sonography is superb when the entire pancreas can be imaged. Unfortunately, even with optimal equipment and scanning technique, the entire pancreas can be visualized in only about _______ of patients. A. 5% to 12% B. 13% to 19% C. 20%% to 25% D. 25% to 50% E. 50% to 65% 2. All of the following statements are true EXCEPT A. Sonography is the primary imaging method used in screening patients with jaundice. B. Sonography is not useful in characterizing abnormalities noted on CT. C. Ultrasound may identify a pancreatic mass in a patient scanned for abdominal pain. D. Ultrasound can usually detect pancreatic carcinoma that obstructs the bile duct. E. Sonography is superb when the entire pancreas can be imaged. 3. Pancreatic ductal adenocarcinoma is by far the most common primary pancreatic neoplasm, comprising approximately _____ of all pancreatic neoplasms. A. 80% B. 70% C. 60% D. 50% E. 40% 4. Which of the following is a true statement? A. Sonographically, pancreatic carcinoma is typically a hyperechoic mass that does not deform the gland's morphology. B. Pancreatic ductal adenocarcinoma is one of the most lethal malignancies, and the overall five-year survival is poor at 30% or less. C. Pancreatic carcinoma, whose prevalence has tripled during the last forty years, is one of the commonest causes of cancer death in the United States. D. Heterogeneous masses are slightly more common than homogeneous masses. E. Masses with increased echogenicity are common in carcinoma but rare in chronic pancreatitis. 5. Slightly more than _____ of pancreatic ductal adenocarcinomas occur in the pancreatic head. A. 20% B. 30% C. 40% D. 60% E. 80% 6. All of the following findings suggest unresectability of pancreatic ductal carcinoma EXCEPT A. tumor less than 2 cm B. extracapsular extension C. vascular invasion (venous or arterial) D. lymphadenopathy E. metastatic disease 7. The five-year survival of patients undergoing attempted curative resection in the more recent studies have reported a range of A. 50% to 60% B. 40% to 50% C. 30% to 40% D. 20% to 30% E. 10% to 20% 8. Regarding carcinoma and masses associated with chronic pancreatitis, all of the following statements are true EXCEPT A. Focal pancreatic enlargement occurs in approximately 30 % of patients with chronic pancreatitis. B. The presence of calcification within a mass makes the diagnosis of pancreatitis certain because carcinomas do not have calcifications. C. Carcinoma and pancreatitis may both cause obstruction of the pancreatic duct or extrahepatic bile duct. D. Carcinoma and chronic pancreatitis related masses can usually be differentiated clinically. E. Pseudocysts, while more frequent in pancreatitis, can occur in both conditions. 9. Cystic pancreatic tumors are relatively uncommon, comprising fewer than ____ of pancreatic cystic lesions and only a few percent of pancreatic tumors. A. 45% B. 35% C. 25% D. 15% E. 5% 10. Regarding serous cystic neoplasms, all of the following are true EXCEPT A. They are almost universally benign. B. C. D. E. When image findings typical for these neoplasms are present, asymptomatic or poor risk patients need not undergo surgery. Another name for these tumors is macrocystic adenoma. They are slightly more common in females and tend to occur in older individuals. A distinctive but inconsistent feature is a central stellate fibrotic scar that frequently calcifies (seen in about 50% of tumors). 11. Regarding mucinous cystic neoplasms, which of the following statements is true? A. They consist of very small cysts that are easily imaged with CT but not by sonography. B. Because differentiation between benign and malignant mucinous cystic neoplasms is often impossible, all tumors are considered malignant and surgical removal is indicated. C. They are much more common in males, approaching a 10 to 1 predominance. D. Most tumors are located in the head of the pancreas. E. Calcifications occur in approximately 50% of these neoplasms (compared to about only 20% in the serous cystic neoplasms). 12. Regarding endocrine tumors, ________ and gastrinomas are the most common. A. glucagonomas B. carcinoid tumors C. somatostatinomas D. pheochromocytoma E. insulinomas 13. All of the following are pancreatic tumors that can originate from the islet cell EXCEPT A. pheochromocytoma B. melanoma C. glucagonoma D. vasoactive intestinal peptide tumor E. somatostatinoma 14. Regarding islet cell tumors, all of the following are true statements EXCEPT A. Published success rates for the detection of insulinomas vary from 25% to 60%. B. Insulinomas and gastrinomas are frequently less than 2 cm in diameter. C. It is relatively easy to image islet cell tumors because they are usually large when the patient presents with hormonal abnormalities. D. Sonographically, islet cell tumors are usually well defined and round or oval in shape. E. They generally appear hypoechoic compared to the normal pancreatic parenchyma. 15. In autopsy series, the most common pancreatic neoplasm is A. combined histology tumor B. C. D. E. ductal adenocarcinoma metastatic carcinoma serous cystic tumor gastrinoma 16. Primary tumors that commonly metastasize to the pancreas include all of the following EXCEPT A. melanoma B. lung cancer C. breast cancer D. stomach cancer E. basal cell cancer 17. Sonography is often the first modality used to image patients with pancreatic carcinoma, as these patients usually present with A. jaundice or abdominal pain. B. vomiting. C. abnormal blood tests. D. an abdominal mass. E. diarrhea. 18. Pancreatic neoplasms tend to be A. non-compressible and are often immobile. B. non-compressible but are often mobile. C. non-visible by ultrasound so compression and mobility are of no use. D. compressible but are often immobile. E. compressible and are often mobile. 19. In the study discussed in this article, a complete technical success sonographically was achieved in _____ of 51 patients. A. 73% B. 79% C. 85% D. 89% E. 96% 20. In the study discussed in the article, a “touch/no touch” color Doppler analysis that compared color Doppler findings to tumor free margins showed that when tumor did not touch vessels, the margins were negative in A. 30 of 30 patients B. 20 of 20 patients C. 15 of 15 patients D. 10 of 10 patients E. 5 of 5 patients